Reizine Natalie, Vokes Everett E, Liu Ping, Truong Tien M, Nanda Rita, Fleming Gini F, Catenacci Daniel V T, Pearson Alexander T, Parsad Sandeep, Danahey Keith, van Wijk Xander M R, Yeo Kiang-Teck J, Ratain Mark J, O'Donnell Peter H
Section of Hematology/Oncology, Department of Medicine, University of Chicago Medical Center and Biological Sciences, Chicago, IL, USA.
Department of Public Health Sciences, University of Chicago, Chicago, IL, USA.
Ther Adv Med Oncol. 2020 Dec 17;12:1758835920974118. doi: 10.1177/1758835920974118. eCollection 2020.
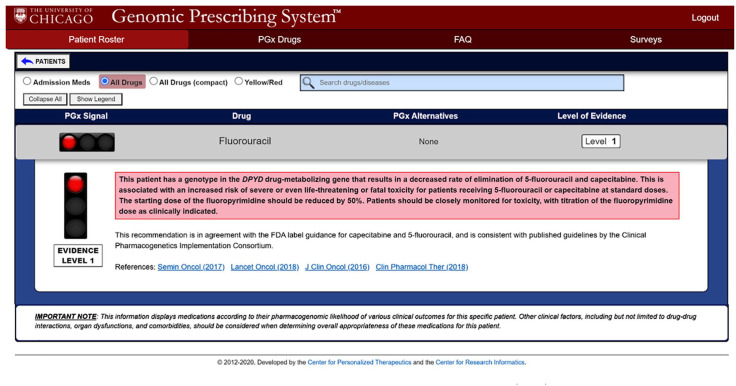
Many cancer patients who receive chemotherapy experience adverse drug effects. Pharmacogenomics (PGx) has promise to personalize chemotherapy drug dosing to maximize efficacy and safety. Fluoropyrimidines and irinotecan have well-known germline PGx associations. At our institution, we have delivered PGx clinical decision support (CDS) based on preemptively obtained genotyping results for a large number of non-oncology medications since 2012, but have not previously evaluated the utility of this strategy for patients initiating anti-cancer regimens. We hypothesize that providing oncologists with preemptive germline PGx information along with CDS will enable individualized dosing decisions and result in improved patient outcomes.
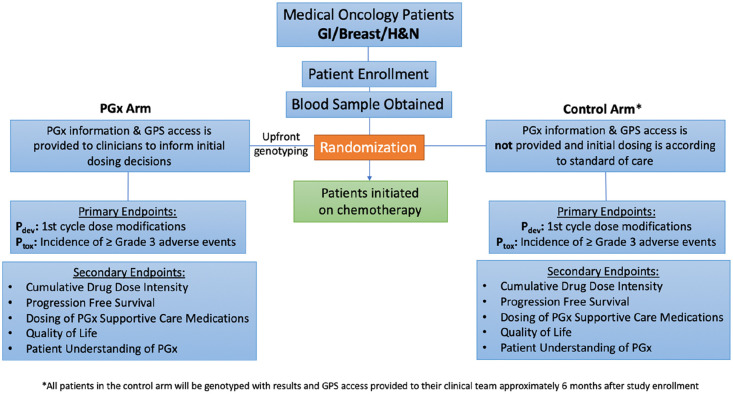
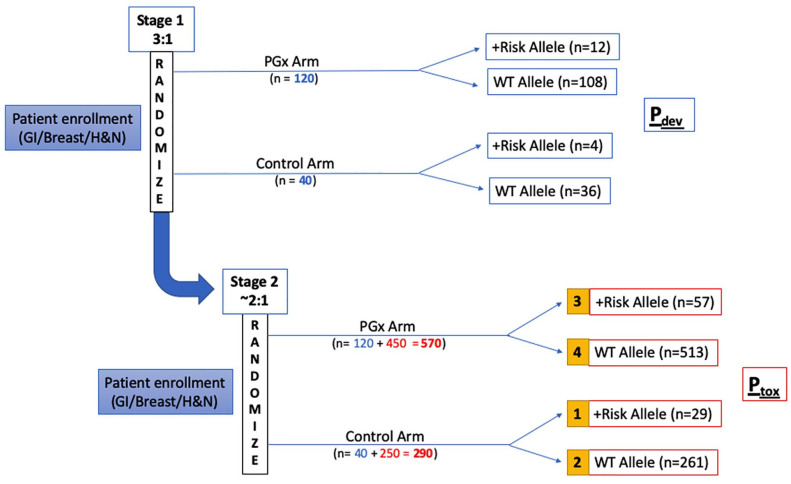
Patients with oncologic malignancies for whom fluoropyrimidine and/or irinotecan-inclusive therapy is being planned will be enrolled and randomly assigned to PGx and control arms. Patients will be genotyped in a clinical laboratory across panels that include actionable variants in and . For PGx arm patients, treating providers will be given access to the patient-specific PGx results with CDS prior to treatment initiation. In the control arm, genotyping will be deferred, and dosing will occur as per usual care. Co-primary endpoints are dose intensity deviation rate (the proportion of patients receiving dose modifications during the first treatment cycle), and grade ⩾3 treatment-related toxicities throughout the treatment course. Additional study endpoints will include cumulative drug dose intensity, progression-free survival, dosing of additional PGx supportive medications, and patient-reported quality of life and understanding of PGx.
Providing a platform of integrated germline PGx information may promote personalized chemotherapy dosing decisions and establish a new model of care to optimize oncology treatment planning.
许多接受化疗的癌症患者会经历药物不良反应。药物基因组学(PGx)有望实现化疗药物剂量的个体化,以最大限度地提高疗效和安全性。氟嘧啶和伊立替康具有众所周知的种系PGx关联。自2012年以来,在我们机构,我们基于预先获得的大量非肿瘤药物的基因分型结果提供PGx临床决策支持(CDS),但此前尚未评估该策略对开始抗癌治疗方案患者的效用。我们假设,为肿瘤学家提供预先的种系PGx信息以及CDS将有助于做出个体化的给药决策,并改善患者预后。
计划接受含氟嘧啶和/或伊立替康治疗的肿瘤恶性肿瘤患者将被纳入研究,并随机分配到PGx组和对照组。患者将在临床实验室进行基因分型,检测包括[具体基因名称1]和[具体基因名称2]中可操作变异的多个基因 panel。对于PGx组患者,治疗提供者将在治疗开始前获得患者特异性的PGx结果及CDS。在对照组中,基因分型将推迟,给药将按照常规护理进行。共同主要终点是剂量强度偏差率(在第一个治疗周期内接受剂量调整的患者比例),以及整个治疗过程中≥3级的治疗相关毒性。其他研究终点将包括累积药物剂量强度、无进展生存期、额外PGx支持性药物的给药情况,以及患者报告的生活质量和对PGx的理解。
提供一个整合的种系PGx信息平台可能会促进个体化化疗给药决策,并建立一种新的护理模式,以优化肿瘤治疗计划。