Department of Radiology, Reims University Hospital, 51092 Reims, France.
Clinical Research Department, Reims University Hospital, 51092 Reims, France.
Diagn Interv Imaging. 2021 Feb;102(2):77-84. doi: 10.1016/j.diii.2020.12.002. Epub 2020 Dec 17.
The purpose of this study was to identify clinical and chest computed tomography (CT) features associated with a severe form of coronavirus disease 2019 (COVID-19) and to propose a quick and easy to use model to identify patients at risk of a severe form.
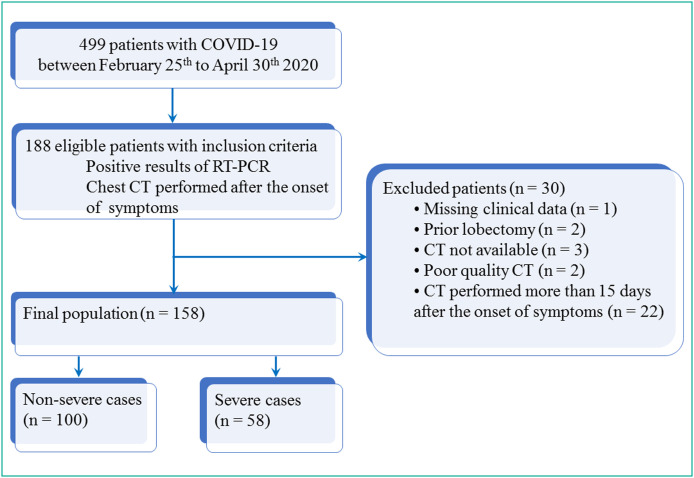
A total of 158 patients with biologically confirmed COVID-19 who underwent a chest CT after the onset of the symptoms were included. There were 84 men and 74 women with a mean age of 68±14 (SD) years (range: 24-96years). There were 100 non-severe and 58 severe cases. Their clinical data were recorded and the first chest CT examination was reviewed using a computerized standardized report. Univariate and multivariate analyses were performed in order to identify the risk factors associated with disease severity. Two models were built: one was based only on qualitative CT features and the other one included a semi-quantitative total CT score to replace the variable representing the extent of the disease. Areas under the ROC curves (AUC) of the two models were compared with DeLong's method.
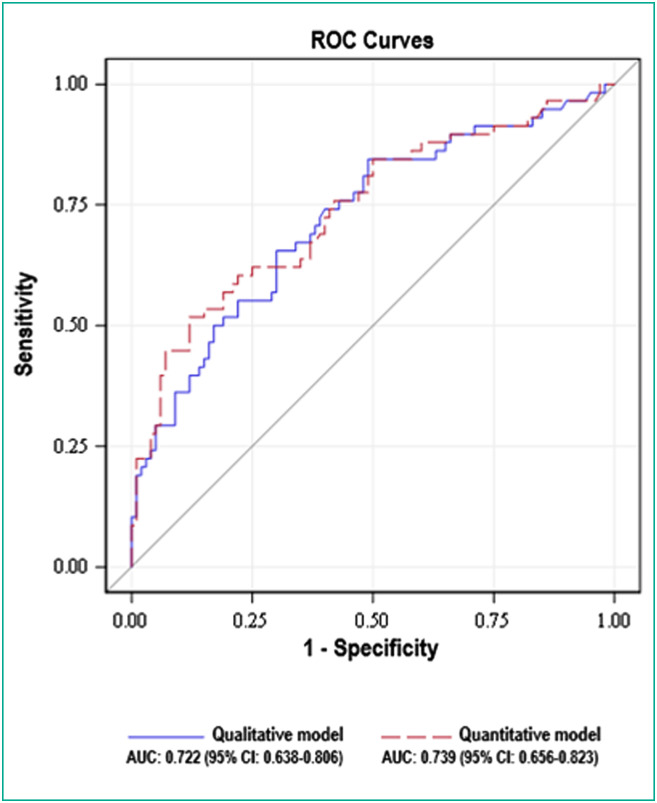
Central involvement of lung parenchyma (P<0.001), area of consolidation (P<0.008), air bronchogram sign (P<0.001), bronchiectasis (P<0.001), traction bronchiectasis (P<0.011), pleural effusion (P<0.026), large involvement of either one of the upper lobes or of the middle lobe (P<0.001) and total CT score≥15 (P<0.001) were more often observed in the severe group than in the non-severe group. No significant differences were found between the qualitative model (large involvement of either upper lobes or middle lobe [odd ratio (OR)=2.473], central involvement [OR=2.760], pleural effusion [OR=2.699]) and the semi-quantitative model (total CT score≥15 [OR=3.342], central involvement [OR=2.344], pleural effusion [OR=2.754]) with AUC of 0.722 (95% CI: 0.638-0.806) vs. 0.739 (95% CI: 0.656-0.823), respectively (P=0.209).
We have developed a new qualitative chest CT-based multivariate model that provides independent risk factors associated with severe form of COVID-19.
本研究旨在确定与 2019 年冠状病毒病(COVID-19)严重形式相关的临床和胸部计算机断层扫描(CT)特征,并提出一种快速易用的模型来识别有严重形式风险的患者。
共纳入 158 例经生物学证实的 COVID-19 患者,这些患者在症状出现后均接受了胸部 CT 检查。其中男性 84 例,女性 74 例,平均年龄 68±14(SD)岁(范围:24-96 岁)。100 例为非重症病例,58 例为重症病例。记录了他们的临床数据,并使用计算机化的标准化报告对首次胸部 CT 检查进行了回顾。进行了单变量和多变量分析,以确定与疾病严重程度相关的危险因素。建立了两个模型:一个仅基于定性 CT 特征,另一个模型则包含半定量总 CT 评分来代替代表疾病程度的变量。使用 DeLong 方法比较了两个模型的 ROC 曲线下面积(AUC)。
肺部实质中央受累(P<0.001)、实变区面积(P<0.008)、空气支气管征(P<0.001)、支气管扩张(P<0.001)、牵拉性支气管扩张(P<0.011)、胸腔积液(P<0.026)、单侧上叶或中叶的大受累(P<0.001)和总 CT 评分≥15(P<0.001)在重症组中比在非重症组中更常见。定性模型(单侧上叶或中叶大受累[比值比(OR)=2.473]、中央受累[OR=2.760]、胸腔积液[OR=2.699])和半定量模型(总 CT 评分≥15[OR=3.342]、中央受累[OR=2.344]、胸腔积液[OR=2.754])与 AUC 为 0.722(95%CI:0.638-0.806)和 0.739(95%CI:0.656-0.823),分别为 0.722(95%CI:0.638-0.806)和 0.739(95%CI:0.656-0.823)(P=0.209),之间无显著差异。
我们开发了一种新的基于胸部 CT 的多变量定性模型,提供了与 COVID-19 严重形式相关的独立危险因素。