Edet Angela, Ku Katherine, Guzman Irene, Dargham Hanadi Abou
St. Joseph Medical Center, 1800 N California Street, Stockton, California 95204, USA.
Touro University College of Osteopathic Medicine, 1310 Club Drive, Vallejo, California 94592, USA.
Case Rep Crit Care. 2020 Dec 22;2020:6616805. doi: 10.1155/2020/6616805. eCollection 2020.
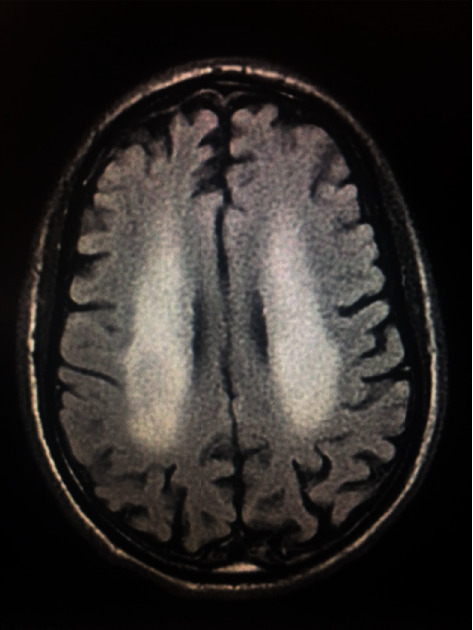
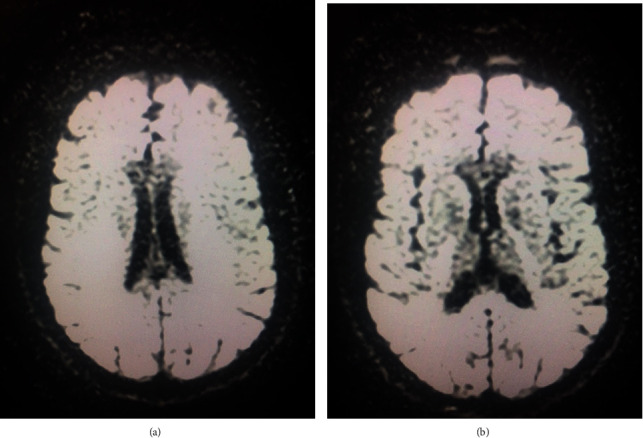
A 32-year-old male presented to the emergency department (ED) with a productive cough for 4 days and confusion for 2 days prior to presentation. He was febrile, tachycardic, and hypotensive. Initially, labs and influenza A/B PCR were performed. An elevated WBC of 17.3 and a lactate level of 3.1 were noted. He was given a bolus of normal saline and broad spectrum antibiotics, ceftriaxone and azithromycin. The patient was then subsequently found to be positive for influenza A via rapid antigen testing of the nares. On hospital day 2, the patient's mental status and respiratory distress worsened requiring intubation with mechanical ventilation. CT of the head without contrast revealed symmetric areas of hypoattenuation in the frontoparietal deep white matter. Lumbar puncture showed a slight elevation in WBCs and mild lymphocytic pleocytosis. Brain MRI without contrast revealed symmetric hyperintense T2 FLAIR signaling in the periventricular white matter and the splenium of the corpus callosum. He was found to have encephalitis secondary to influenza A and was started on a course of oseltamivir at higher doses of 150 mg BID for 2 weeks. On hospital day 10, after nine days of intubation, the patient received a tracheostomy due to failure to extubate and no improvement in mental status. He remained ventilator-dependent with little improvement in mental status; the patient was transferred to a long-term acute care hospital (LTACH) facility for further specialized care. He did not show any neurologic recovery or improvement in the three months after initial presentation of symptoms. In the fifth month after the initial symptoms, there was no recovery of preinsult neurologic function. The family had a palliative care meeting to discuss the plan and goals of care. It was decided by close family members that "compassionate extubation" would be done due to ongoing stress on the patient's body physically and neurologically. This case illustrates the importance of prompt identification and treatment of influenza in the prevention of rapidly progressive sequelae.
一名32岁男性因咳嗽4天、就诊前2天出现意识模糊而被送至急诊科。他发热、心动过速且血压降低。最初,进行了实验室检查及甲型/乙型流感病毒聚合酶链反应(PCR)检测。白细胞计数升高至17.3,乳酸水平为3.1。给予他一剂生理盐水及广谱抗生素头孢曲松和阿奇霉素。随后通过鼻腔快速抗原检测发现该患者甲型流感呈阳性。住院第2天,患者的精神状态和呼吸窘迫加重,需要进行气管插管并机械通气。头颅CT平扫显示额顶叶深部白质有对称的低密度区。腰椎穿刺显示白细胞略有升高,轻度淋巴细胞增多。头颅磁共振成像(MRI)平扫显示脑室周围白质和胼胝体压部有对称的T2液体衰减反转恢复(FLAIR)高信号。他被诊断为甲型流感继发脑炎,并开始接受高剂量(150毫克,每日两次)的奥司他韦治疗,疗程为2周。住院第10天,在插管9天后,由于无法拔管且精神状态无改善,患者接受了气管造口术。他仍依赖呼吸机,精神状态改善甚微;患者被转至长期急性护理医院(LTACH)接受进一步的专科护理。在最初出现症状后的三个月内,他未表现出任何神经功能恢复或改善。在最初症状出现后的第五个月,病前神经功能仍未恢复。家属召开了姑息治疗会议,讨论护理计划和目标。近亲决定,鉴于患者身体和神经方面持续承受的压力,将进行“同情性拔管”。本病例说明了及时识别和治疗流感在预防快速进展性后遗症方面的重要性。