Srichawla Bahadar S
Department of Neurology, University of Massachusetts Chan Medical School, Worcester, USA.
Cureus. 2022 Oct 25;14(10):e30681. doi: 10.7759/cureus.30681. eCollection 2022 Oct.
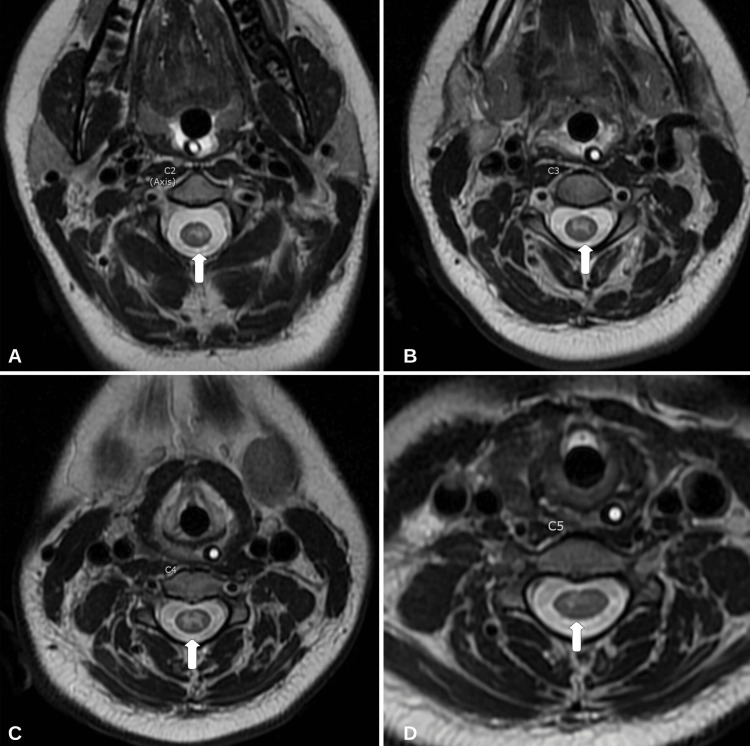
Mild encephalopathy/encephalitis with a reversible splenial lesion (MERS) and longitudinally extensive transverse myelitis (LETM) are neuroinflammatory conditions related to the brain and spinal cord, respectively. Most cases of MERS and LETM are related to a secondary autoimmune process in response to an initial insult (i.e., infection, immunization, etc.). The case of an 18-year-old female who developed a three-day history of fever, quadriplegia, cough, and mild encephalopathy is reported here. The patient tested positive for influenza B by nasopharyngeal swab with polymerase chain reaction (PCR). Initial magnetic resonance imaging (MRI) revealed the presence of a diffusion-restricted non-enhancing lesion confined to the splenium of the corpus callosum (MERS type I) and longitudinally extensive non-enhancing T2 hyperintensities from C1 to C5. The patient was managed with a five-day course of 1,000 mg of intravenous methylprednisolone (IVMP). Additionally, five days of therapeutic plasmapheresis (PLEX) was completed. The patient showed significant improvement with medical management and physical therapy. At the one-year follow-up, her motor symptoms had resolved and endorsed only mild paresthesia in the upper extremities. A repeat MRI revealed a reversal of the splenium lesion and moderate improvement in T2 hyperintensities of the cervical cord. Assessing neuroinvasion of the influenza virus is difficult, and diagnostic challenges arise in determining primary infectious versus autoimmune-mediated neuroinflammation. A review of the literature on influenza infection with radiographic findings of MERS and LETM is included.
伴有可逆性胼胝体压部病变的轻度脑病/脑炎(MERS)和纵向广泛横贯性脊髓炎(LETM)分别是与脑和脊髓相关的神经炎症性疾病。大多数MERS和LETM病例与对初始损伤(即感染、免疫接种等)的继发性自身免疫过程有关。本文报告了一名18岁女性的病例,该患者出现了为期三天的发热、四肢瘫痪、咳嗽和轻度脑病症状。患者经鼻咽拭子聚合酶链反应(PCR)检测乙型流感呈阳性。初始磁共振成像(MRI)显示胼胝体压部存在一个扩散受限的无强化病变(I型MERS),以及从C1到C5的纵向广泛无强化T2高信号。患者接受了为期五天的1000毫克静脉注射甲泼尼龙(IVMP)治疗。此外,还完成了五天的治疗性血浆置换(PLEX)。患者在药物治疗和物理治疗后有显著改善。在一年的随访中,她的运动症状已消失,仅上肢有轻度感觉异常。复查MRI显示胼胝体压部病变逆转,颈髓T2高信号中度改善。评估流感病毒的神经侵袭很困难,在确定原发性感染与自身免疫介导的神经炎症方面存在诊断挑战。本文还对流感感染伴MERS和LETM影像学表现的文献进行了综述。