Siempos Ilias I, Xourgia Eleni, Ntaidou Theodora K, Zervakis Dimitris, Magira Eleni E, Kotanidou Anastasia, Routsi Christina, Zakynthinos Spyros G
First Department of Critical Care Medicine and Pulmonary Services, Evangelismos Hospital, National and Kapodistrian University of Athens Medical School, Athens, Greece.
Division of Pulmonary and Critical Care Medicine, Department of Medicine, New York-Presbyterian Hospital-Weill Cornell Medical Center, Weill Cornell Medicine, New York, NY, United States.
Front Med (Lausanne). 2020 Dec 23;7:614152. doi: 10.3389/fmed.2020.614152. eCollection 2020.
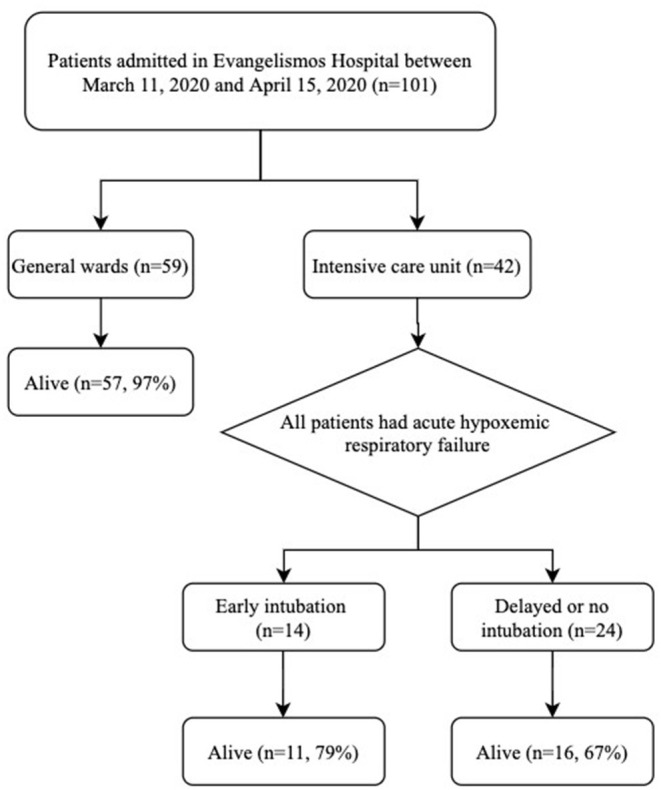
Optimal timing of initiation of invasive mechanical ventilation in patients with acute hypoxemic respiratory failure due to COVID-19 is unknown. Thanks to early flattening of the epidemiological curve, ventilator demand in Greece was kept lower than supply throughout the pandemic, allowing for unbiased comparison of the outcomes of patients undergoing early intubation vs. delayed or no intubation. We conducted an observational study including all adult patients with laboratory-confirmed COVID-19 consecutively admitted in Evangelismos Hospital, Athens, Greece between March 11, 2020 and April 15, 2020. Patients subsequently admitted in the intensive care unit (ICU) were categorized into the "early intubation" vs. the "delayed or no intubation" group. The "delayed or no intubation" group included patients receiving non-rebreather mask for equal to or more than 24 h or high-flow nasal oxygen for any period of time or non-invasive mechanical ventilation for any period of time in an attempt to avoid intubation. The remaining intubated patients comprised the "early intubation" group. During the study period, a total of 101 patients (37% female, median age 65 years) were admitted in the hospital. Fifty-nine patients (58% of the entire cohort) were exclusively hospitalized in general wards with a mortality of 3% and median length of stay of 7 days. Forty-two patients (19% female, median age 65 years) were admitted in the ICU; all with acute hypoxemic respiratory failure. Of those admitted in the ICU, 62% had at least one comorbidity and 14% were never intubated. Early intubation was not associated with higher ICU-mortality (21 vs. 33%), fewer ventilator-free days (3 vs. 2 days) or fewer ICU-free days than delayed or no intubation. A strategy of early intubation was not associated with worse clinical outcomes compared to delayed or no intubation. Given that early intubation may presumably reduce virus aerosolization, these results may justify further research with a randomized controlled trial.
新型冠状病毒肺炎(COVID-19)所致急性低氧性呼吸衰竭患者开始有创机械通气的最佳时机尚不清楚。由于疫情流行曲线提前趋于平缓,在整个疫情期间,希腊对呼吸机的需求一直低于供应水平,这使得我们能够对早期插管与延迟插管或不插管患者的结局进行无偏倚比较。我们开展了一项观察性研究,纳入了2020年3月11日至2020年4月15日期间连续入住希腊雅典埃万杰利斯塔斯医院且实验室确诊为COVID-19的所有成年患者。随后入住重症监护病房(ICU)的患者被分为“早期插管”组和“延迟或不插管”组。“延迟或不插管”组包括接受无重复呼吸面罩通气至少24小时、或接受任何时长的高流量鼻导管给氧、或接受任何时长的无创机械通气以避免插管的患者。其余插管患者组成“早期插管”组。在研究期间,共有101例患者(37%为女性,中位年龄65岁)入院。59例患者(占整个队列的58%)仅在普通病房住院,死亡率为3% , 中位住院时间为7天。42例患者(19%为女性,中位年龄65岁)入住ICU;均为急性低氧性呼吸衰竭。在入住ICU的患者中,62%至少有一种合并症,14%从未插管。与延迟或不插管相比,早期插管与更高的ICU死亡率(21%对33%)、更少的无呼吸机天数(3天对2天)或更少的无ICU天数无关。与延迟或不插管相比,早期插管策略与更差的临床结局无关。鉴于早期插管可能会减少病毒气溶胶的产生,这些结果可能为进一步开展随机对照试验提供依据。