Maggio Julie, Alluri Priyanka R, Paredes-Echeverri Sara, Larson Anna G, Sojka Petr, Price Bruce H, Aybek Selma, Perez David L
Functional Neurology Research Group, Cognitive Behavioral Neurology Unit, Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Department of Psychiatry, University Hospital Brno, Czech Republic.
Brain Commun. 2020 Sep 23;2(2):fcaa156. doi: 10.1093/braincomms/fcaa156. eCollection 2020.
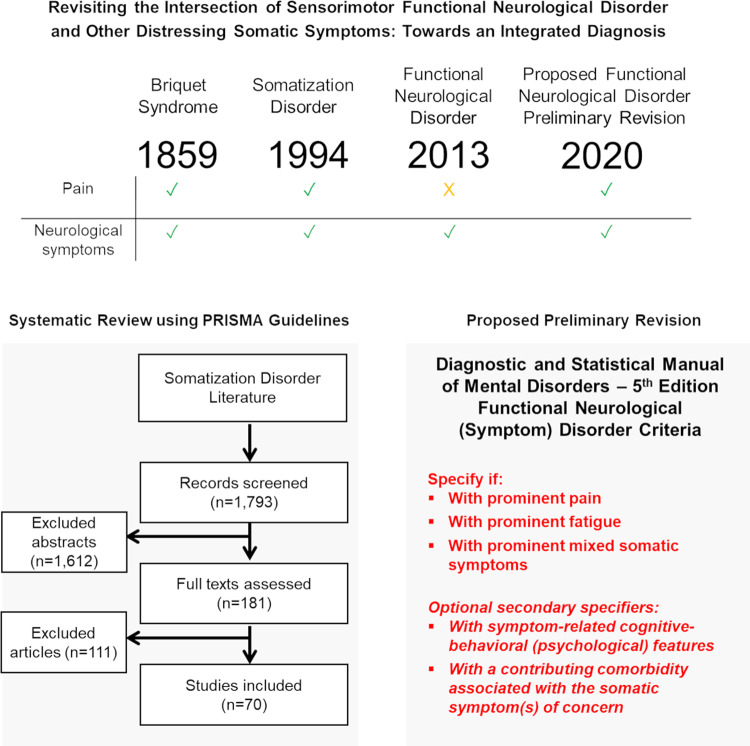
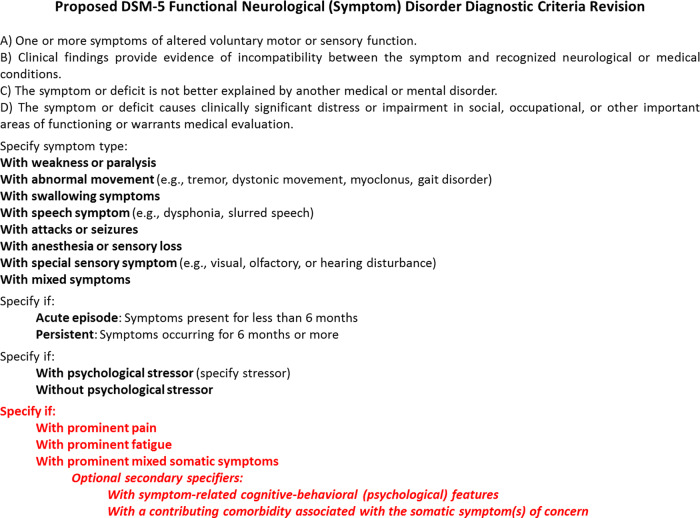
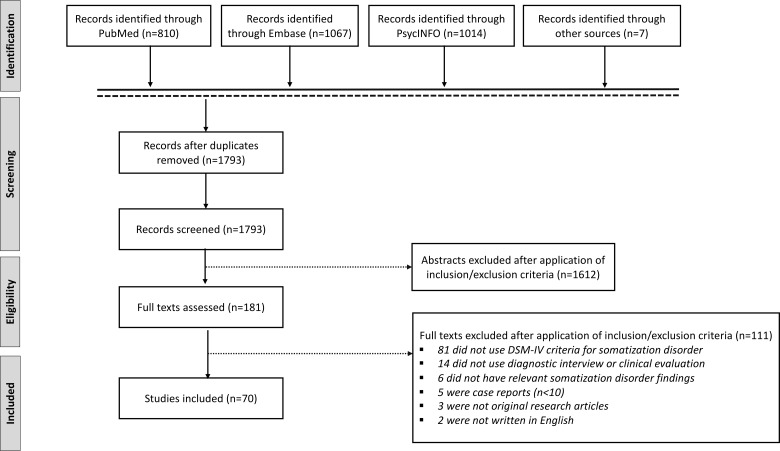
With the creation of the Somatic Symptom and Related Disorders category of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition in 2013, the functional neurological (symptom) disorder diagnostic criteria underwent transformative changes. These included an emphasis on 'rule-in' physical examination signs/semiological features guiding diagnosis and the removal of a required proximal psychological stressor to be linked to symptoms. In addition, the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition somatization disorder, somatoform pain disorder and undifferentiated somatoform disorder conditions were eliminated and collapsed into the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition somatic symptom disorder diagnosis. With somatic symptom disorder, emphasis was placed on a cognitive-behavioural (psychological) formulation as the basis for diagnosis in individuals reporting distressing bodily symptoms such as pain and/or fatigue; the need for bodily symptoms to be 'medically unexplained' was removed, and the overall utility of this diagnostic criteria remains debated. A consequence of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition restructuring is that the diagnosis of somatization disorder that encompassed individuals with functional neurological (sensorimotor) symptoms prominent other bodily symptoms, including pain, was eliminated. This change negatively impacts clinical and research efforts because many patients with functional neurological disorder experience pain, supporting that the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition would benefit from an integrated diagnosis at this intersection. We seek to revisit this with modifications, particularly since pain (and a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition somatization disorder comorbidity, more specifically) is associated with poor clinical prognosis in functional neurological disorder. As a first step, we systematically reviewed the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition somatization disorder literature to detail epidemiologic, healthcare utilization, demographic, diagnostic, medical and psychiatric comorbidity, psychosocial, neurobiological and treatment data. Thereafter, we propose a preliminary revision to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition allowing for the specifier functional neurological disorder 'with prominent pain'. To meet this criterion, core functional neurological symptoms (e.g. limb weakness, gait difficulties, seizures, non-dermatomal sensory loss and/or blindness) would have 'rule-in' signs pain (>6 months) impairing social and/or occupational functioning would also be present. Two optional secondary specifiers assist in characterizing individuals with cognitive-behavioural (psychological) features recognized to amplify or perpetuate pain and documenting if there is a pain-related comorbidity. The specifier of 'with prominent pain' is etiologically neutral, while secondary specifiers provide additional clarification. We advocate for a similar approach to contextualize fatigue and mixed somatic symptoms in functional neurological disorder. While this preliminary proposal requires prospective data and additional discussion, these revisions offer the potential benefit to readily identify important functional neurological disorder subgroups-resulting in diagnostic, treatment and pathophysiology implications.
随着2013年《精神疾病诊断与统计手册》第五版中躯体症状及相关障碍类别的创立,功能性神经(症状)障碍的诊断标准经历了变革性的变化。这些变化包括强调用于指导诊断的“纳入”体格检查体征/症状学特征,以及不再要求有与症状相关的近期心理应激源。此外,《精神疾病诊断与统计手册》第四版中的躯体化障碍、躯体形式疼痛障碍和未分化躯体形式障碍被取消,并合并为《精神疾病诊断与统计手册》第五版中的躯体症状障碍诊断。对于躯体症状障碍,重点在于以认知行为(心理)构成为报告疼痛和/或疲劳等令人痛苦的躯体症状的个体进行诊断的基础;不再要求躯体症状“无法用医学解释”,并且该诊断标准的整体效用仍存在争议。《精神疾病诊断与统计手册》第五版结构调整的一个后果是,涵盖具有突出的功能性神经(感觉运动)症状以及包括疼痛在内的其他躯体症状的个体的躯体化障碍诊断被取消。这一变化对临床和研究工作产生了负面影响,因为许多功能性神经障碍患者会经历疼痛,这表明《精神疾病诊断与统计手册》第五版在这一交叉领域采用综合诊断将有益处。我们试图对此进行修改后重新审视,特别是因为疼痛(更具体地说,以及与《精神疾病诊断与统计手册》第四版中的躯体化障碍共病)与功能性神经障碍的不良临床预后相关。作为第一步,我们系统回顾了《精神疾病诊断与统计手册》第四版中躯体化障碍的文献,以详细阐述流行病学、医疗保健利用、人口统计学、诊断、医学和精神科共病、心理社会、神经生物学和治疗数据。此后,我们对《精神疾病诊断与统计手册》第五版提出了初步修订建议,允许使用“伴有突出疼痛”的功能性神经障碍说明符。要符合这一标准,核心功能性神经症状(如肢体无力、步态困难、癫痫发作、非皮节性感觉丧失和/或失明)将有“纳入”体征,并且还会存在疼痛(超过6个月),损害社会和/或职业功能。两个可选的次要说明符有助于描述具有被认为会放大或使疼痛持续存在的认知行为(心理)特征的个体,并记录是否存在与疼痛相关的共病。“伴有突出疼痛”的说明符在病因上是中性的,而次要说明符提供了更多的澄清。我们主张采用类似的方法来界定功能性神经障碍中的疲劳和混合躯体症状。虽然这一初步提议需要前瞻性数据和更多讨论,但这些修订有可能带来好处,即能够轻松识别重要的功能性神经障碍亚组,从而产生诊断、治疗和病理生理学方面的影响。