Environmental Health and Engineering, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland, USA
Environmental Health and Engineering, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland, USA.
BMJ Open. 2021 Jan 13;11(1):e043528. doi: 10.1136/bmjopen-2020-043528.
To evaluate associations of community types and features with new onset type 2 diabetes in diverse communities. Understanding the location and scale of geographic disparities can lead to community-level interventions.
Nested case-control study within the open dynamic cohort of health system patients.
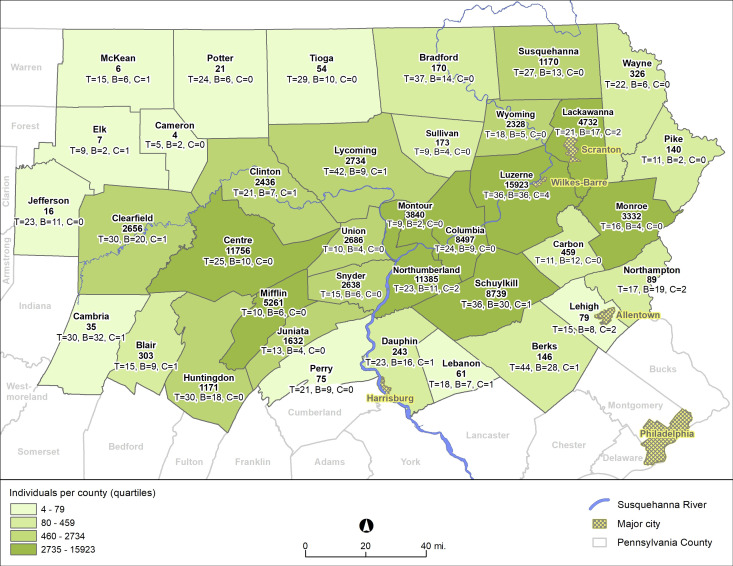
Large, integrated health system in 37 counties in central and northeastern Pennsylvania, USA.
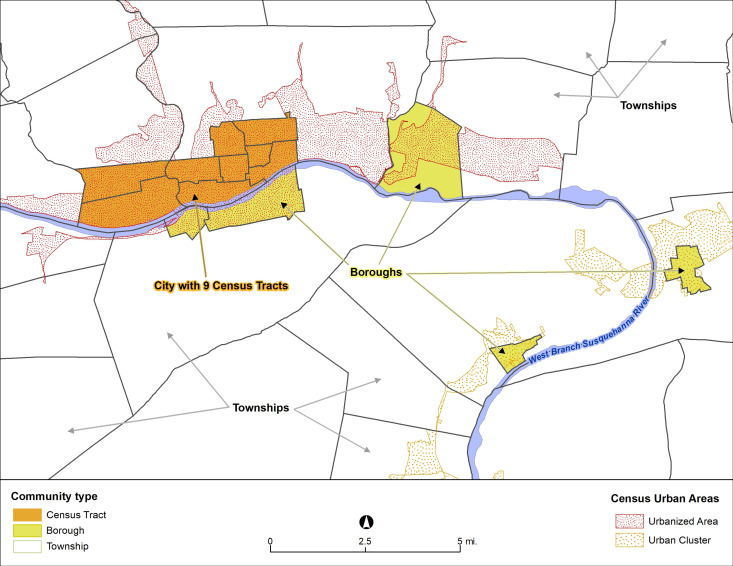
We used electronic health records to identify persons with new-onset type 2 diabetes from 2008 to 2016 (n=15 888). Persons with diabetes were age, sex and year matched (1:5) to persons without diabetes (n=79 435). We used generalised estimating equations to control for individual-level confounding variables, accounting for clustering of persons within communities. Communities were defined as (1) townships, boroughs and city census tracts; (2) urbanised area (large metro), urban cluster (small cities and towns) and rural; (3) combination of the first two; and (4) county. Community socioeconomic deprivation and greenness were evaluated alone and in models stratified by community types.
Borough and city census tract residence (vs townships) were associated (OR (95% CI)) with higher odds of type 2 diabetes (1.10 (1.04 to 1.16) and 1.34 (1.25 to 1.44), respectively). Urbanised areas (vs rural) also had increased odds of type 2 diabetes (1.14 (1.08 to 1.21)). In the combined definition, the strongest associations (vs townships in rural areas) were city census tracts in urban clusters (1.41 (1.22 to 1.62)) and city census tracts in urbanised areas (1.33 (1.22 to 1.45)). Higher community socioeconomic deprivation and lower greenness were each associated with increased odds.
Urban residence was associated with higher odds of type 2 diabetes than for other areas. Higher community socioeconomic deprivation in city census tracts and lower greenness in all community types were also associated with type 2 diabetes.
评估不同社区的社区类型和特征与 2 型糖尿病新发病例之间的关联。了解地理差异的位置和规模可以促进社区层面的干预。
健康系统患者开放动态队列中的嵌套病例对照研究。
美国宾夕法尼亚州中北部 37 个县的大型综合卫生系统。
我们使用电子健康记录从 2008 年至 2016 年确定新诊断的 2 型糖尿病患者(n=15888)。将糖尿病患者与无糖尿病患者(n=79435)按年龄、性别和年份进行 1:5 匹配。我们使用广义估计方程来控制个体水平的混杂变量,同时考虑到社区内个体的聚类。社区定义为(1)城镇、自治市镇和城市普查区;(2)城市化区域(大城市)、城市化集群(小城市和城镇)和农村;(3)前两者的组合;以及(4)县。社区社会经济贫困程度和绿化程度单独评估,并按社区类型分层模型进行评估。
与乡镇相比,自治市镇和城市普查区的居住(OR(95%CI))与 2 型糖尿病的更高发病几率相关(1.10(1.04 至 1.16)和 1.34(1.25 至 1.44))。城市化地区(与农村地区相比)也增加了 2 型糖尿病的发病几率(1.14(1.08 至 1.21))。在联合定义中,与乡镇在农村地区相比,最强的关联是城市普查区在城市化集群中的(1.41(1.22 至 1.62))和城市普查区在城市化地区中的(1.33(1.22 至 1.45))。社区社会经济贫困程度较高和绿化程度较低与发病几率增加相关。
与其他地区相比,城市居住与 2 型糖尿病的发病几率较高相关。城市普查区的社区社会经济贫困程度较高和所有社区类型的绿化程度较低与 2 型糖尿病也有关联。