Shabbir Asad, Camm Christian Fielder, Elkington Andrew, Tilling Lindsey, Stirrup James, Chan Antoni, Bull Sacha
The Royal Berkshire Hospital, London Road, Reading RG1 5AN, UK.
Eur Heart J Case Rep. 2020 Oct 30;4(6):1-6. doi: 10.1093/ehjcr/ytaa370. eCollection 2020 Dec.
Concurrent myopericarditis and myositis can present in patients with pre-existing systemic inflammatory diseases. Here we present a case of myopericarditis and myositis associated with COVID-19, in the absence of respiratory symptoms.
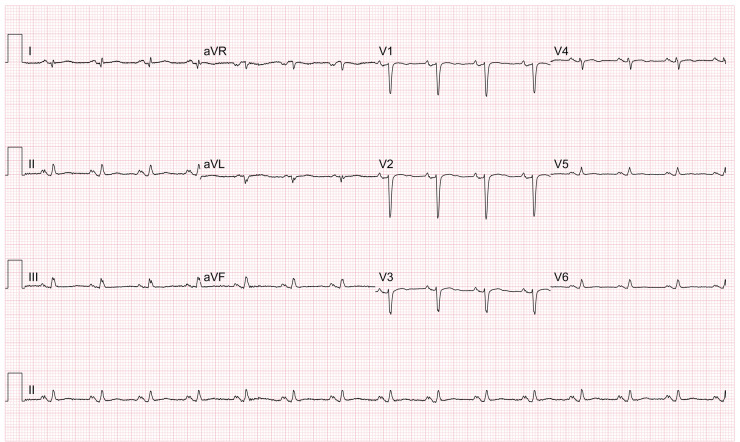
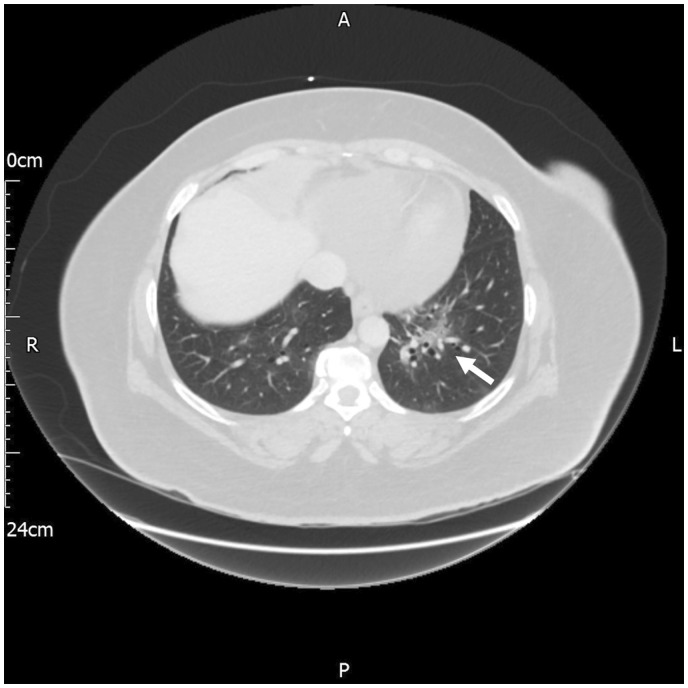
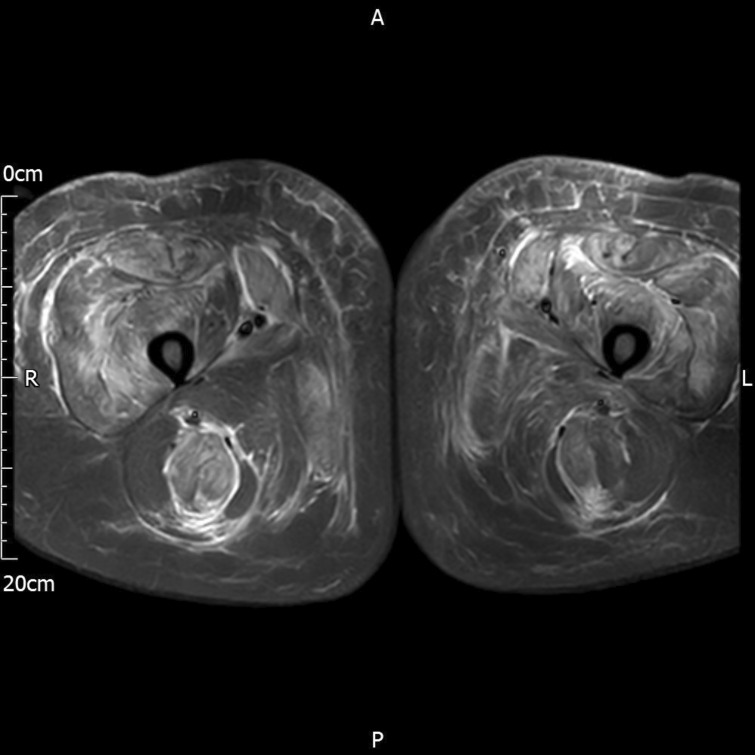
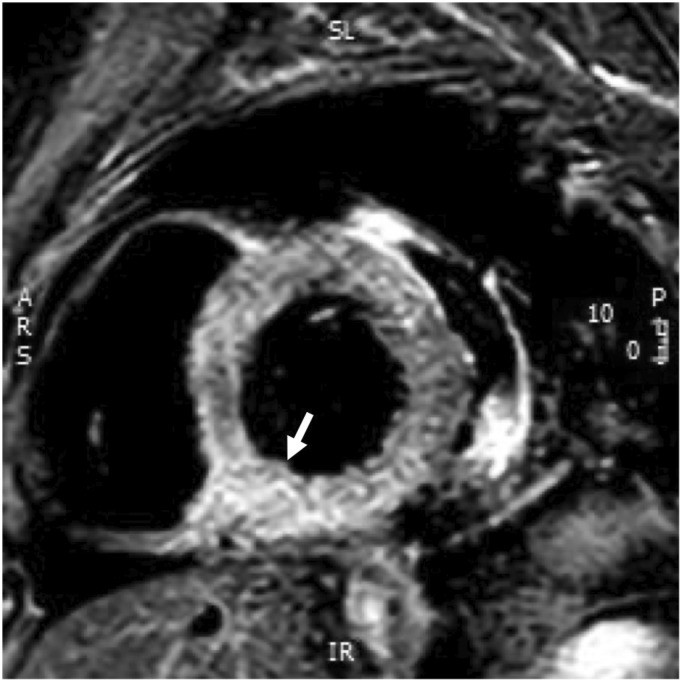
We present a middle-aged female with a history of hypertension and previous myopericarditis. The patient was admitted with symptoms of central chest pain, and ECG and echocardiographic features of myopericarditis. Her symptoms did not improve, and CT thorax suggested possible SARS-CoV-2 infection for which she tested positive, despite no respiratory symptoms. Whilst on the ward, she developed bilateral leg weakness and a raised creatine kinase (CK), and magnetic resonance imaging (MRI) of her thighs confirmed myositis. A cardiac MRI confirmed myopericarditis. She was treated with colchicine 500 μg twice daily, ibuprofen 400 mg three times day, and prednisolone 30 mg per day, and her symptoms and weakness improved.
We describe the first reported case of concurrent myopericarditis, and myositis associated with COVID-19. Conventional therapy with colchicine, non-steroidal anti-inflammatory drugs, and glucocorticoids improved her symptoms, and reduced biochemical markers of myocardial and skeletal muscle inflammation.
合并性心肌心包炎和肌炎可出现在患有全身性炎症性疾病的患者中。在此,我们报告一例与2019冠状病毒病(COVID-19)相关的心肌心包炎和肌炎病例,该患者无呼吸道症状。
我们报告一名中年女性,有高血压病史且既往有心肌心包炎。患者因胸痛症状入院,心电图和超声心动图显示有心肌心包炎特征。尽管没有呼吸道症状,但她的症状未改善,胸部CT提示可能感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2),检测结果呈阳性。在病房期间,她出现双侧腿部无力,肌酸激酶(CK)升高,大腿磁共振成像(MRI)证实为肌炎。心脏MRI证实为心肌心包炎。她接受了秋水仙碱每日两次、每次500μg,布洛芬每日三次、每次400mg,以及泼尼松龙每日30mg的治疗,症状和无力情况有所改善。
我们描述了首例报告的与COVID-19相关的合并性心肌心包炎和肌炎病例。秋水仙碱、非甾体抗炎药和糖皮质激素的常规治疗改善了她的症状,并降低了心肌和骨骼肌炎症的生化指标。