Unité de Formation et de Recherche Biosciences, Université Félix Houphouët-Boigny, Abidjan, Côte d'Ivoire.
Centre Suisse de Recherches Scientifiques en Côte d'Ivoire, Abidjan, Côte d'Ivoire.
PLoS Negl Trop Dis. 2021 Jan 15;15(1):e0008845. doi: 10.1371/journal.pntd.0008845. eCollection 2021 Jan.
Preventive chemotherapy using praziquantel is the mainstay for schistosomiasis control. However, there is little evidence on what is supposed to be the most effective school-based treatment strategy to sustain morbidity control. The aim of this study was to compare differences in Schistosoma mansoni prevalence and infection intensity between three different schedules of school-based preventive chemotherapy in an area with moderate prevalence of S. mansoni in Côte d'Ivoire.
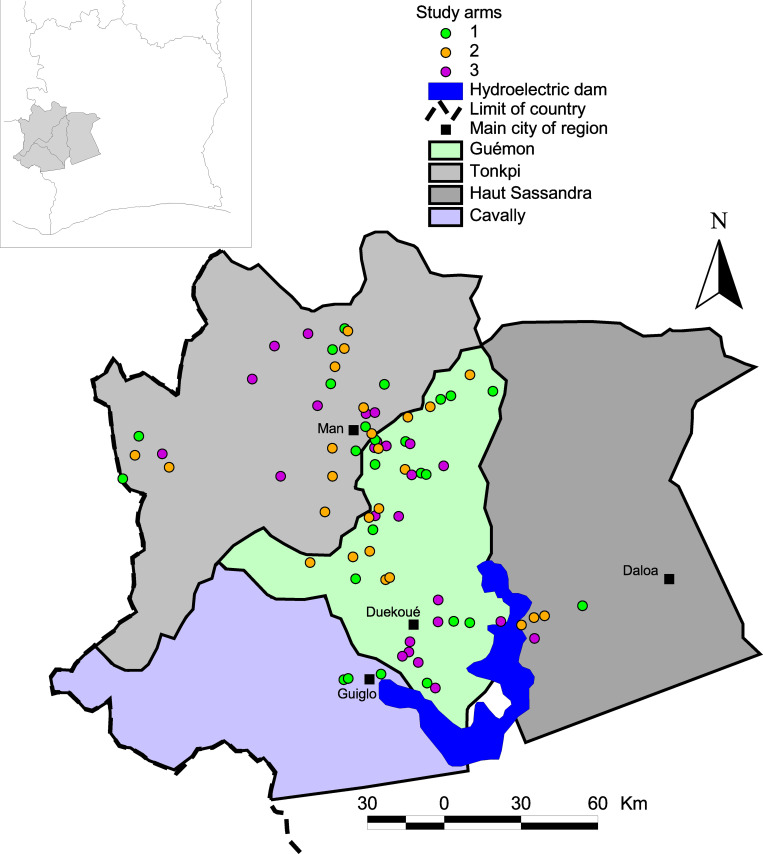
Seventy-five schools were randomly assigned to one of three intervention arms: (i) annual school-based preventive chemotherapy with praziquantel (40 mg/kg) over four years; (ii) praziquantel treatment only in the first two years, followed by two years whithout treatment; and (iii) praziquantel treatment in years 1 and 3 without treatment in-between. Cross-sectional parasitologic surveys were carried out prior to each round of preventive chemotherapy. The difference in S. mansoni prevalence and infection intensity was assessed by multiple Kato-Katz thick smears, among children aged 9-12 years at the time of each survey. First-grade children, aged 5-8 years who had never received praziquantel, were also tested at baseline and at the end of the study.
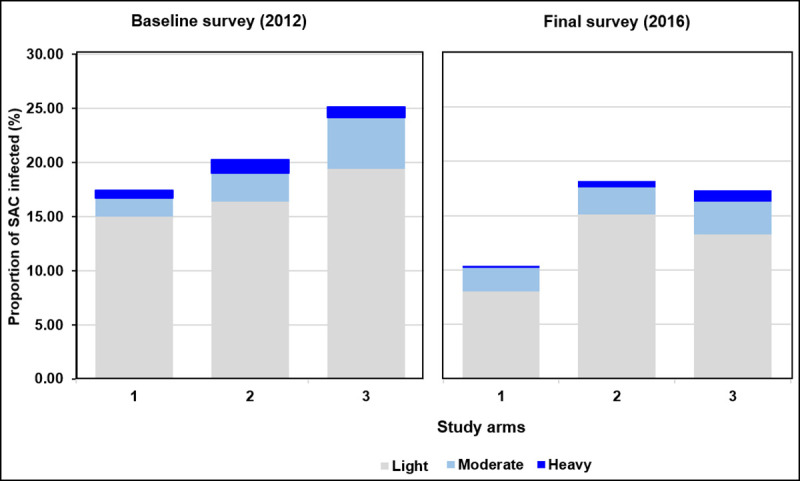
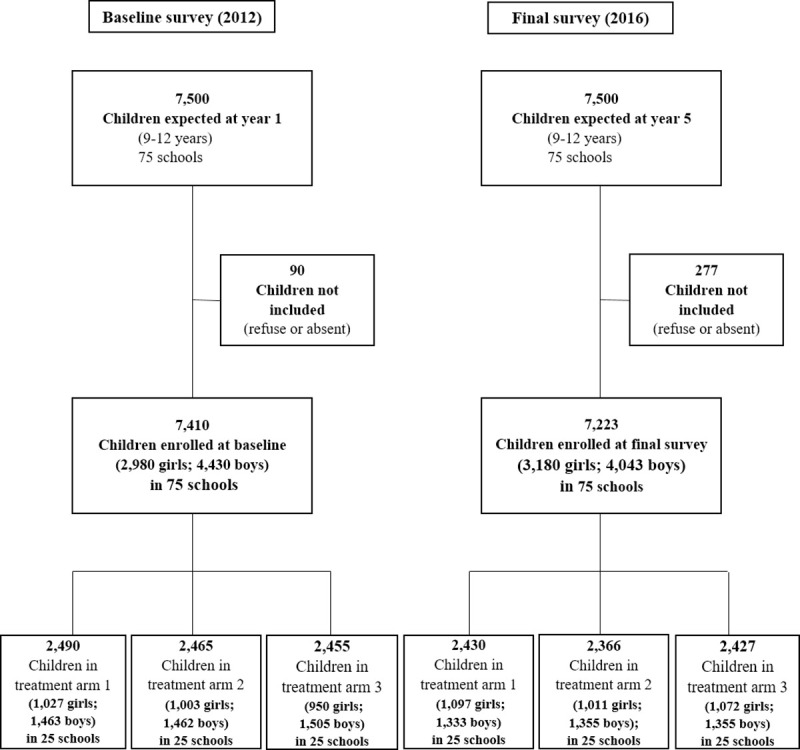
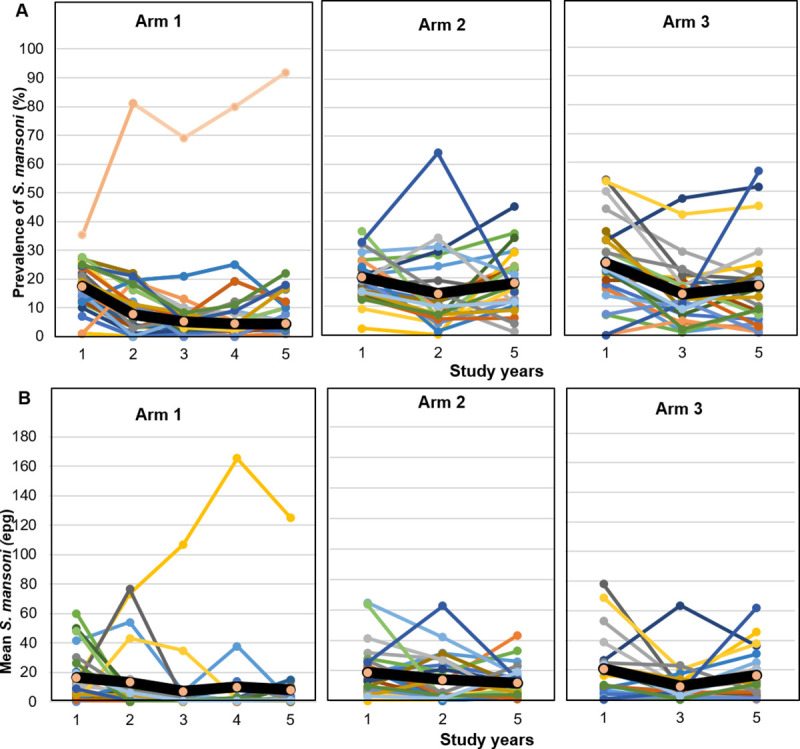
Overall, 7,410 children aged 9-12 years were examined at baseline and 7,223 at the final survey. The baseline prevalence of S. mansoni was 17.4%, 20.2%, and 25.2% in arms 1, 2, and 3, respectively. In the final year, we observed the lowest prevalence of 10.4% in arm 1, compared to 18.2% in arm 2 and 17.5% in arm 3. The comparison between arms 1 and 2 estimated an odds ratio (OR) of 0.52 but the difference was not statistically significant (95% confidence interval (CI) = 0.23-1.16). Likewise the difference between arms 1 and 3 lacked statistical significance (OR = 0.55, 95% CI = 0.23-1.29). There was no noteworthy difference observed between arms 2 and 3 (OR = 1.06, 95% CI = 0.64-1.75). The lowest S. mansoni fecal egg counts in the final year survey were observed in arm 1 (7.9 eggs per gram of stool (EPG)). However, compared with 11.5 EPG in arm 2 and 15.4 EPG in arm 3, the difference lacked statistical significance. There were 4,812 first-grade children examined at baseline and 4,513 in the final survey. The overall prevalence of S. mansoni in these children slightly decreased in arms 1 (from 4.5% to 3.6%) and 2 (from 4.7% to 4.3%), but increased in arm 3 (from 6.8% to 7.9%). However, there was no significant difference in prevalence and infection intensity observed between study arms.
CONCLUSIONS/SIGNIFICANCE: The three treatment schedules investigated led to a reduction in the prevalence and intensity of S. mansoni infection among children aged 9-12 years. Comparing intervention arms at the end of the study, no statistically significant differences were observed between annual treatement and the other two treatment schedules, neither in reduction of prevalence nor intensity of infection. It is important to combine our results with those of three sister trials conducted simultaneously in other African countries, before final recommendations can be drawn.
使用吡喹酮进行预防性化疗是血吸虫病控制的主要手段。然而,对于维持发病率控制应该采用哪种最有效的基于学校的治疗策略,几乎没有证据。本研究的目的是比较在科特迪瓦中曼氏血吸虫流行率中等地区的三种不同基于学校的预防性化疗方案之间曼氏血吸虫的患病率和感染强度的差异。
75 所学校被随机分配到三个干预组之一:(i)在四年内每年进行基于学校的预防性化疗,剂量为 40mg/kg;(ii)前两年仅给予吡喹酮治疗,随后两年不治疗;(iii)在第 1 年和第 3 年给予吡喹酮治疗,中间两年不治疗。在每轮预防性化疗前进行横断面寄生虫学调查。通过对 9-12 岁儿童进行多次加藤厚涂片检查,评估曼氏血吸虫的患病率和感染强度的差异。在基线和研究结束时还对从未接受过吡喹酮治疗的 5-8 岁一年级儿童进行了检测。
共有 7410 名 9-12 岁儿童在基线和最后一次调查时接受了检查,7223 名儿童在最后一次调查时接受了检查。第 1 组、第 2 组和第 3 组的曼氏血吸虫基线患病率分别为 17.4%、20.2%和 25.2%。在最后一年,我们观察到第 1 组的患病率最低,为 10.4%,而第 2 组和第 3 组的患病率分别为 18.2%和 17.5%。第 1 组与第 2 组之间的比较估计了一个优势比(OR)为 0.52,但差异无统计学意义(95%置信区间(CI)为 0.23-1.16)。同样,第 1 组与第 3 组之间的差异也没有统计学意义(OR=0.55,95%CI=0.23-1.29)。第 2 组和第 3 组之间没有观察到显著差异(OR=1.06,95%CI=0.64-1.75)。在最后一年的调查中,第 1 组的曼氏血吸虫粪便卵计数最低(每克粪便 7.9 个虫卵(EPG))。然而,与第 2 组的 11.5 EPG 和第 3 组的 15.4 EPG 相比,差异无统计学意义。共有 4812 名一年级儿童在基线时接受了检查,4513 名儿童在最后一次调查时接受了检查。这些儿童的曼氏血吸虫总患病率在第 1 组(从 4.5%降至 3.6%)和第 2 组(从 4.7%降至 4.3%)略有下降,但在第 3 组(从 6.8%升至 7.9%)有所上升。然而,各组之间的患病率和感染强度均无显著差异。
结论/意义:三种治疗方案均导致 9-12 岁儿童的曼氏血吸虫感染的患病率和感染强度降低。在研究结束时对干预组进行比较,在降低患病率和感染强度方面,年度治疗与其他两种治疗方案之间均无统计学差异。在得出最终建议之前,将我们的结果与同时在其他非洲国家进行的三项姐妹试验的结果结合起来非常重要。