Kyroudi A, Petersson K, Ozsahin E, Bourhis J, Bochud F, Moeckli R
Institute of Radiation Physics, Lausanne University Hospital, Rue du Grand-Pré 1, CH 1007 Lausanne, Switzerland.
Department of Radiation Oncology, Lausanne University Hospital, Rue du Bugnon 46, CH 1011 Lausanne, Switzerland.
Phys Imaging Radiat Oncol. 2020 Jun 12;14:82-86. doi: 10.1016/j.phro.2020.05.008. eCollection 2020 Apr.
Radiotherapy treatment planning is a multi-criteria problem. Any optimization of the process produces a set of mathematically optimal solutions. These optimal plans are considered mathematically equal, but they differ in terms of the trade-offs involved. Since the various objectives are conflicting, the choice of the best plan for treatment is dependent on the preferences of the radiation oncologists or the medical physicists (decision makers).We defined a clinically relevant area on a prostate Pareto front which better represented clinical preferences and determined if there were differences among radiation oncologists and medical physicists.
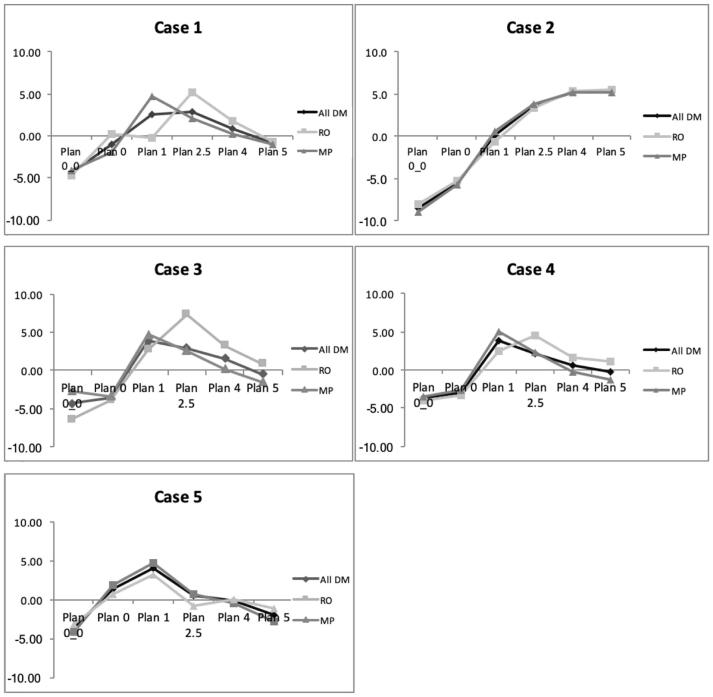
Pareto fronts of five localized prostate cancer patients were used to analyze and visualize the trade-off between the rectum sparing and the PTV under-dosage. Clinical preferences were evaluated with Clinical Grading Analysis by asking nine radiation oncologists and ten medical physicists to rate pairs of plans presented side by side. A choice of the optimal plan on the Pareto front was made by all decision makers.
The plans in the central region of the Pareto front (1-4% PTV under-dosage) received the best evaluations. Radiation oncologists preferred the organ at risk (OAR) sparing region (2.5-4% PTV under-dosage) while medical physicists preferred better PTV coverage (1-2.5% PTV under-dosage). When the Pareto fronts were additionally presented to the decisions makers they systematically chose the plan in the trade-off region (0.5-1% PTV under-dosage).
We determined a specific region on the Pareto front preferred by the radiation oncologists and medical physicists and found a difference between them.
放射治疗计划是一个多标准问题。该过程的任何优化都会产生一组数学上的最优解。这些最优计划在数学上被认为是相等的,但它们在涉及的权衡方面有所不同。由于各种目标相互冲突,选择最佳治疗计划取决于放射肿瘤学家或医学物理学家(决策者)的偏好。我们在前列腺帕累托前沿定义了一个临床相关区域,该区域能更好地代表临床偏好,并确定放射肿瘤学家和医学物理学家之间是否存在差异。
使用五名局限性前列腺癌患者的帕累托前沿来分析和可视化直肠保护与计划靶体积(PTV)剂量不足之间的权衡。通过让九名放射肿瘤学家和十名医学物理学家对并排呈现的计划对进行评分,用临床分级分析来评估临床偏好。所有决策者都在帕累托前沿上选择了最优计划。
帕累托前沿中心区域的计划(PTV剂量不足1 - 4%)获得了最佳评价。放射肿瘤学家更喜欢危及器官(OAR)保护区域(PTV剂量不足2.5 - 4%),而医学物理学家更喜欢更好的PTV覆盖(PTV剂量不足1 - 2.5%)。当向决策者额外展示帕累托前沿时,他们系统地选择了权衡区域的计划(PTV剂量不足0.5 - 1%)。
我们确定了放射肿瘤学家和医学物理学家在帕累托前沿上偏好一的个特定区域,并发现了他们之间的差异。