Department of Cardiology, Daping Hospital, The Third Military Medical University, Chongqing, P.R. China.
Chongqing Key Laboratory for Hypertension Research, Chongqing Cardiovascular Clinical Research Center, Chongqing Institute of Cardiology, Chongqing, P.R. China.
Clin Sci (Lond). 2021 Jan 29;135(2):409-427. doi: 10.1042/CS20201340.
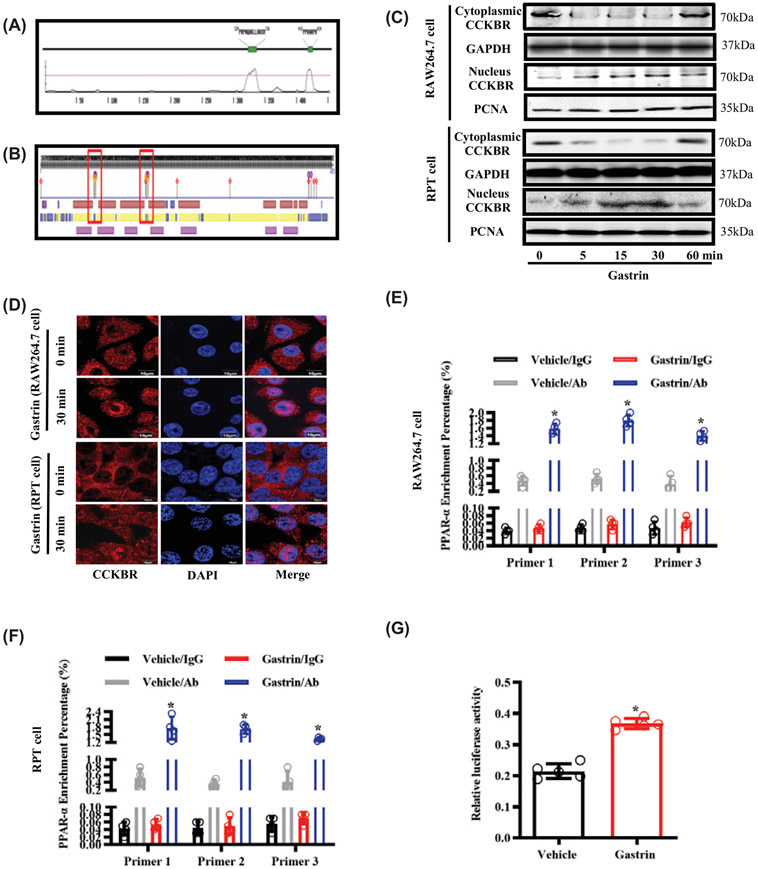
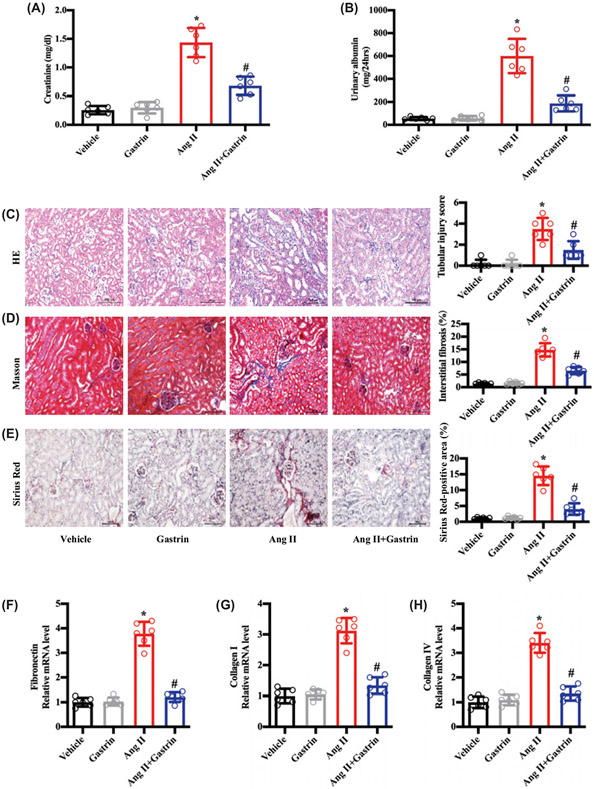
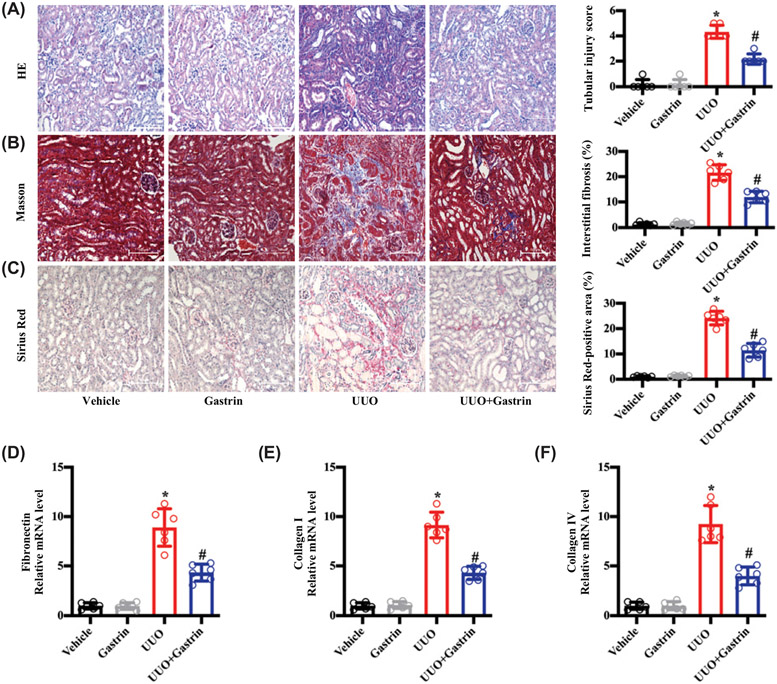
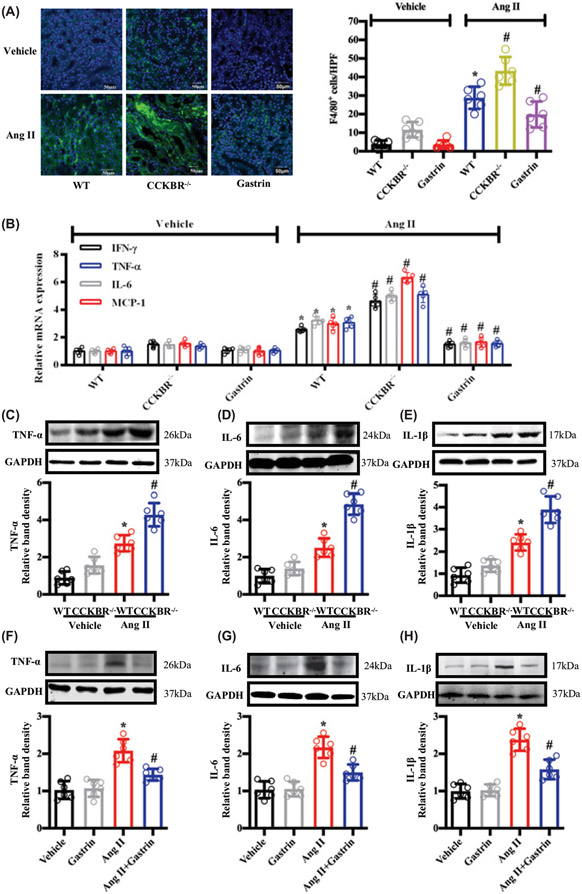
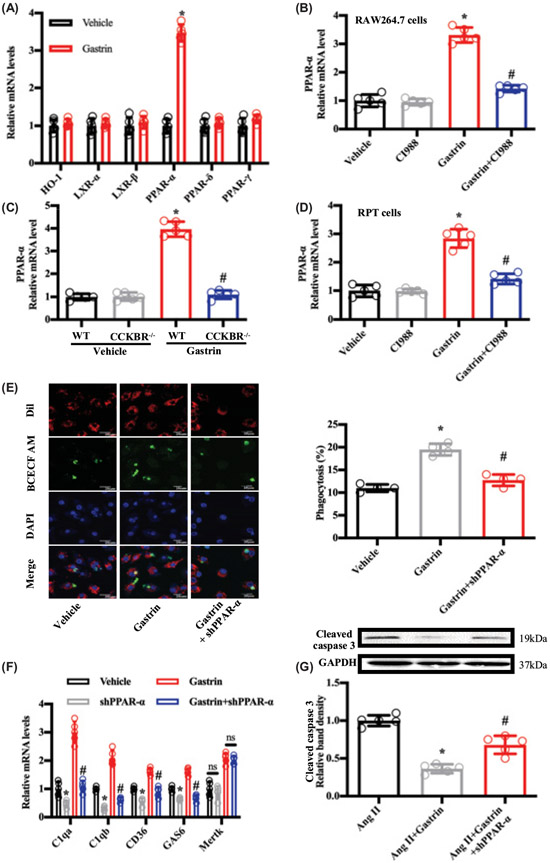
Hypertensive nephropathy (HN) is a common cause of end-stage renal disease with renal fibrosis; chronic kidney disease is associated with elevated serum gastrin. However, the relationship between gastrin and renal fibrosis in HN is still unknown. We, now, report that mice with angiotensin II (Ang II)-induced HN had increased renal cholecystokinin receptor B (CCKBR) expression. Knockout of CCKBR in mice aggravated, while long-term subcutaneous infusion of gastrin ameliorated the renal injury and interstitial fibrosis in HN and unilateral ureteral obstruction (UUO). The protective effects of gastrin on renal fibrosis can be independent of its regulation of blood pressure, because in UUO, gastrin decreased renal fibrosis without affecting blood pressure. Gastrin treatment decreased Ang II-induced renal tubule cell apoptosis, reversed Ang II-mediated inhibition of macrophage efferocytosis, and reduced renal inflammation. A screening of the regulatory factors of efferocytosis showed involvement of peroxisome proliferator-activated receptor α (PPAR-α). Knockdown of PPAR-α by shRNA blocked the anti-fibrotic effect of gastrin in vitro in mouse renal proximal tubule cells and macrophages. Immunofluorescence microscopy, Western blotting, luciferase reporter, and Cut&tag-qPCR analyses showed that CCKBR may be a transcription factor of PPAR-α, because gastrin treatment induced CCKBR translocation from cytosol to nucleus, binding to the PPAR-α promoter region, and increasing PPAR-α gene transcription. In conclusion, gastrin protects against HN by normalizing blood pressure, decreasing renal tubule cell apoptosis, and increasing macrophage efferocytosis. Gastrin-mediated CCKBR nuclear translocation may make it act as a transcription factor of PPAR-α, which is a novel signaling pathway. Gastrin may be a new potential drug for HN therapy.
高血压肾病(HN)是一种常见的终末期肾脏疾病,伴有肾纤维化;慢性肾脏病与血清胃泌素升高有关。然而,胃泌素与 HN 中的肾纤维化之间的关系尚不清楚。我们现在报告,血管紧张素 II(Ang II)诱导的 HN 小鼠的胆囊收缩素受体 B(CCKBR)表达增加。在小鼠中敲除 CCKBR 会加重,而长期皮下输注胃泌素则可改善 HN 和单侧输尿管梗阻(UUO)中的肾损伤和间质纤维化。胃泌素对肾纤维化的保护作用可能与其对血压的调节无关,因为在 UUO 中,胃泌素降低肾纤维化而不影响血压。胃泌素治疗可减少 Ang II 诱导的肾小管细胞凋亡,逆转 Ang II 介导的巨噬细胞吞噬作用抑制,并减少肾脏炎症。对吞噬作用的调节因子的筛选表明涉及过氧化物酶体增殖物激活受体α(PPAR-α)。shRNA 敲低 PPAR-α 可阻断胃泌素在体外对小鼠肾近端小管细胞和巨噬细胞的抗纤维化作用。免疫荧光显微镜、Western blot、荧光素酶报告和 Cut&tag-qPCR 分析表明,CCKBR 可能是 PPAR-α 的转录因子,因为胃泌素处理诱导 CCKBR 从细胞质转位到细胞核,与 PPAR-α 启动子区域结合,并增加 PPAR-α 基因转录。总之,胃泌素通过正常化血压、减少肾小管细胞凋亡和增加巨噬细胞吞噬作用来保护 HN。胃泌素介导的 CCKBR 核转位可能使其作为 PPAR-α 的转录因子发挥作用,这是一种新的信号通路。胃泌素可能是 HN 治疗的一种新的潜在药物。