Department of Obstetrics and Gynecology, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya, 466-8550, Japan.
Division of Public Health Informatics, Department of Integrative Health Science, Nagoya University Graduate School of Medicine, Nagoya, Japan.
Sci Rep. 2021 Jan 18;11(1):1729. doi: 10.1038/s41598-021-81292-7.
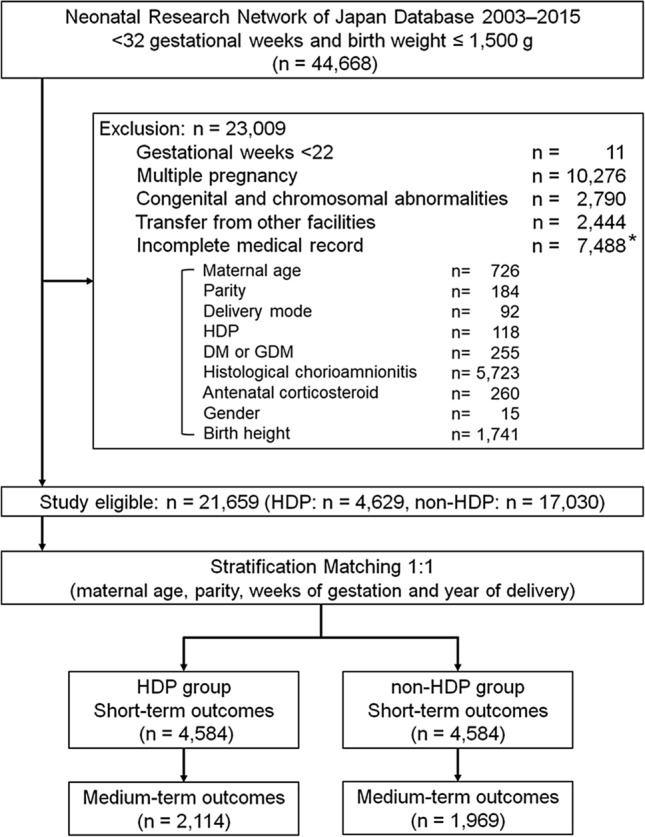
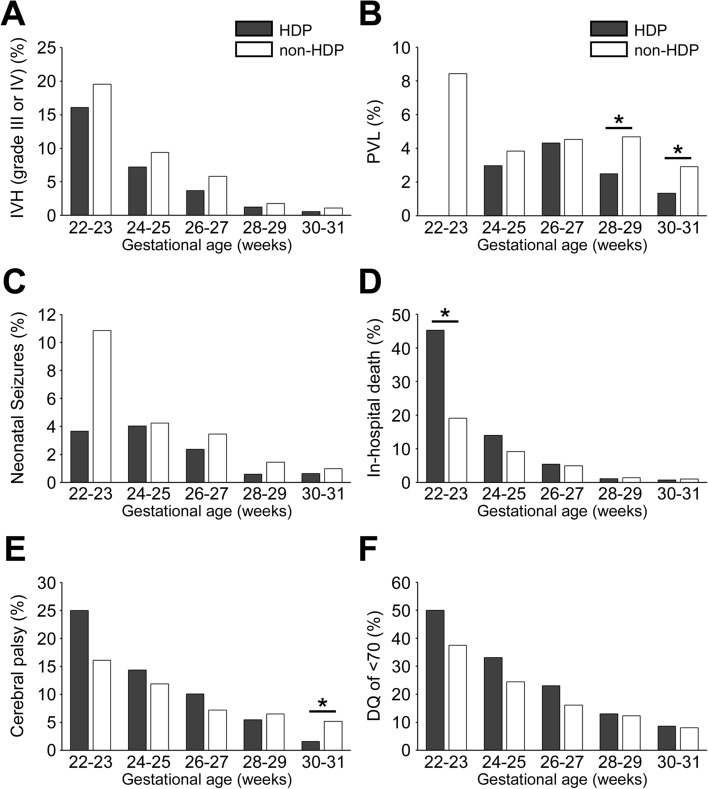
To evaluate the impact of maternal hypertensive disorders of pregnancy (HDP) on mortality and neurological outcomes in extremely and very preterm infants using a nationwide neonatal database in Japan. This population-based retrospective study was based on an analysis of data collected by the Neonatal Research Network of Japan from 2003 to 2015 of neonates weighing 1,500 g or less at birth, between 22 and 31 weeks' gestation. A total of 21,659 infants were randomly divided into two groups, HDP (n = 4,584) and non-HDP (n = 4,584), at a ratio of 1:1 after stratification by four factors including maternal age, parity, weeks of gestation, and year of delivery. Short-term (neonatal period) and medium-term (3 years of age) mortality and neurological outcomes were compared between the two groups by logistic regression analyses. In univariate analysis, HDP was associated with an increased risk for in-hospital death (crude odds ratio [OR], 1.31; 95% confidence interval, 1.04-1.63) and a decreased risk for severe intraventricular haemorrhage (0.68; 0.53-0.87) and periventricular leukomalacia (0.60; 0.48-0.77). In multivariate analysis, HDP was significantly associated with a lower risk for in-hospital death (adjusted OR, 0.61; 0.47-0.80), severe intraventricular haemorrhage (0.47; 0.35-0.63), periventricular leukomalacia (0.59; 0.45-0.78), neonatal seizures (0.40; 0.28-0.57) and cerebral palsy (0.70; 0.52-0.95) at 3 years after adjustment for covariates including birth weight. These results were consistent with those of additional analyses, which excluded cases with histological chorioamnionitis and which divided the infants into two subgroups (22-27 gestational weeks and 28-31 gestational weeks). Maternal HDP was associated with an increased risk for in-hospital death without adjusting for covariates, but it was also associated with a lower risk for mortality and adverse neurological outcomes in extremely and very preterm infants if all covariates except HDP were identical.
利用日本全国新生儿数据库评估母亲妊娠高血压疾病(HDP)对极早产儿和极早产儿死亡和神经结局的影响。本基于人群的回顾性研究基于日本新生儿研究网络(Neonatal Research Network of Japan) 2003 年至 2015 年期间收集的数据进行分析,纳入的新生儿出生体重为 1500g 或以下,胎龄为 22 周至 31 周。共有 21659 名婴儿随机分为 HDP(n=4584)和非 HDP(n=4584)两组,在按母亲年龄、产次、胎龄和分娩年份等四个因素分层后,两组比例为 1:1。通过 logistic 回归分析比较两组短期(新生儿期)和中期(3 岁)死亡率和神经结局。单因素分析显示,HDP 与院内死亡风险增加相关(粗比值比 [OR],1.31;95%置信区间,1.04-1.63),与严重脑室出血(0.68;0.53-0.87)和脑室周围白质软化(0.60;0.48-0.77)风险降低相关。多因素分析显示,HDP 与院内死亡风险显著降低相关(调整 OR,0.61;0.47-0.80)、严重脑室出血(0.47;0.35-0.63)、脑室周围白质软化(0.59;0.45-0.78)、新生儿癫痫发作(0.40;0.28-0.57)和脑瘫(0.70;0.52-0.95)的风险降低相关,这些结果在调整包括出生体重在内的协变量后仍然一致。这些结果与排除组织学绒毛膜羊膜炎病例和将婴儿分为两个亚组(22-27 孕周和 28-31 孕周)的进一步分析结果一致。在不调整协变量的情况下,HDP 与院内死亡风险增加相关,但如果除 HDP 外的所有协变量均相同,HDP 与极早产儿和极早产儿的死亡率和不良神经结局风险降低相关。