Department of Haematology and Phase 1 Unit, Rigshospitalet, Copenhagen, Denmark.
Manchester Academic Health Science Centre, University of Manchester and the Christie NHS Foundation Trust, Manchester, UK.
Hematol Oncol. 2021 Apr;39(2):185-195. doi: 10.1002/hon.2838. Epub 2021 Feb 16.
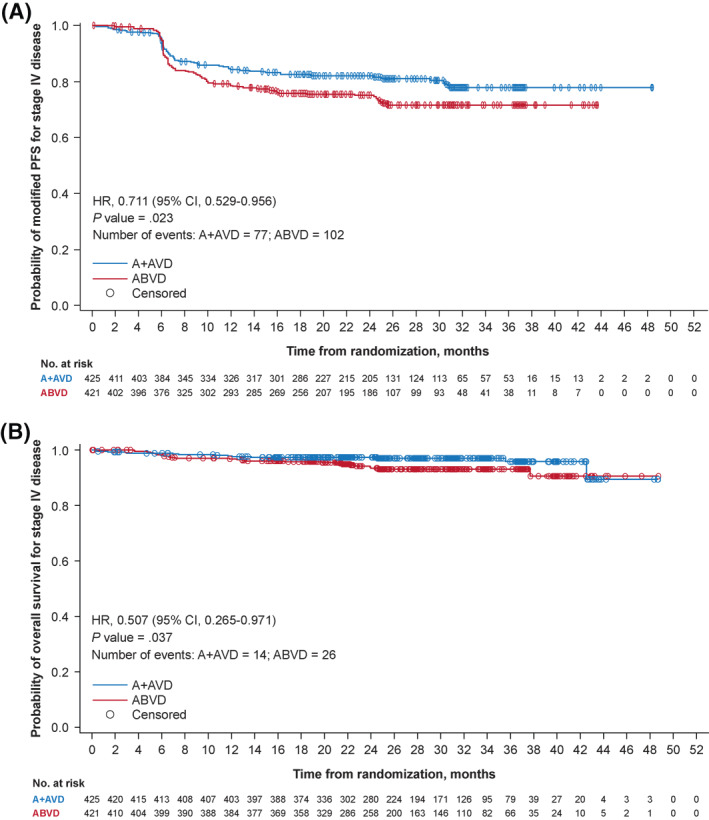
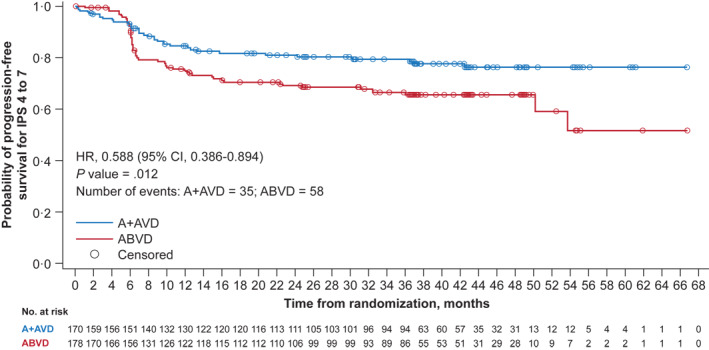
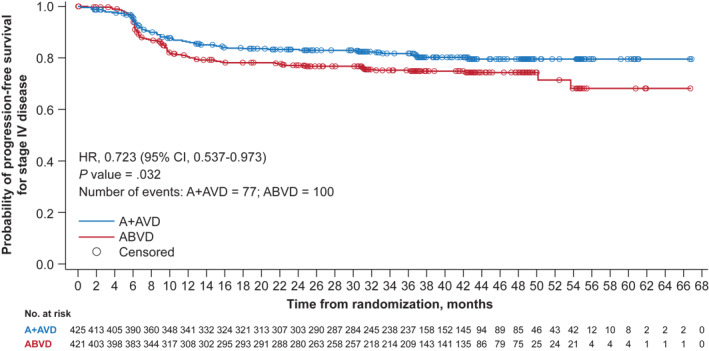
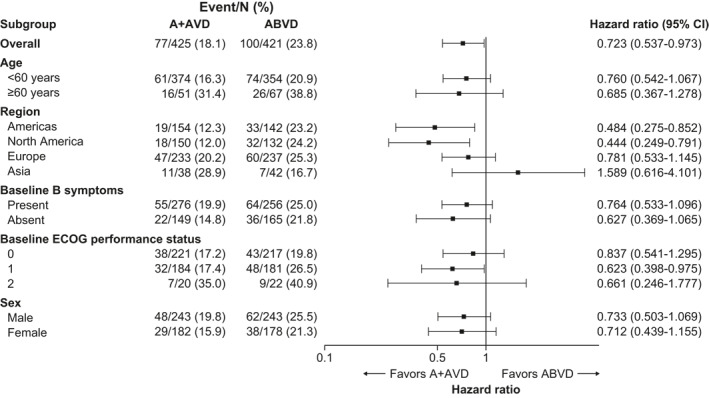
Approximately one-third of patients diagnosed with Hodgkin lymphoma presenting with Stage IV disease do not survive past 5 years. We present updated efficacy and safety analyses in high-risk patient subgroups, defined by Stage IV disease or International Prognostic Score (IPS) of 4-7, enrolled in the ECHELON-1 study that compared brentuximab vedotin plus doxorubicin, vinblastine, and dacarbazine (A + AVD) versus doxorubicin, bleomycin, vinblastine, and dacarbazine (ABVD) as first-line therapy after a median follow-up of 37.1 months. Among patients treated with A + AVD (n = 664) or ABVD (n = 670), 64% had Stage IV disease and 26% had an IPS of 4-7. Patients with Stage IV disease treated with A + AVD showed consistent improvements in PFS at 3 years as assessed by investigator (hazard ratio [HR], 0.723; 95% confidence interval [CI], 0.537-0.973; p = 0.032). Similar improvements were seen in the subgroup of patients with IPS of 4-7 (HR, 0.588; 95% CI, 0.386-0.894; p = 0.012). The most common adverse events (AEs) in A + AVD-treated versus ABVD-treated patients with Stage IV disease were peripheral neuropathy (67% vs. 40%) and neutropenia (71% vs. 55%); in patients with IPS of 4-7, the most common AEs were peripheral neuropathy (69% vs. 45%), neutropenia (66% vs. 55%), and febrile neutropenia (23% vs. 9%), respectively. Patients in high-risk subgroups did not experience greater AE incidence or severity than patients in the total population. This updated analysis of ECHELON-1 shows a favorable benefit-risk balance in high-risk patients.
约三分之一的 IV 期霍奇金淋巴瘤患者在 5 年后无法存活。我们在 ECHELON-1 研究中报告了高危患者亚组的更新疗效和安全性分析,该研究比较了 brentuximab vedotin 联合多柔比星、长春碱和达卡巴嗪(A+AVD)与多柔比星、博来霉素、长春碱和达卡巴嗪(ABVD)作为一线治疗,中位随访 37.1 个月后。在接受 A+AVD(n=664)或 ABVD(n=670)治疗的患者中,64%患有 IV 期疾病,26%的国际预后评分(IPS)为 4-7。接受 A+AVD 治疗的 IV 期疾病患者的 PFS 在 3 年时得到一致改善,由研究者评估(风险比[HR],0.723;95%置信区间[CI],0.537-0.973;p=0.032)。在 IPS 为 4-7 的亚组患者中也观察到类似的改善(HR,0.588;95%CI,0.386-0.894;p=0.012)。在 IV 期疾病患者中,与 ABVD 相比,接受 A+AVD 治疗的患者最常见的不良反应(AE)为周围神经病(67% vs. 40%)和中性粒细胞减少症(71% vs. 55%);在 IPS 为 4-7 的患者中,最常见的 AE 为周围神经病(69% vs. 45%)、中性粒细胞减少症(66% vs. 55%)和发热性中性粒细胞减少症(23% vs. 9%)。高危亚组患者的 AE 发生率或严重程度并未高于总人群。ECHELON-1 的这项更新分析显示高危患者的获益风险平衡良好。