School of Medicine and Public Health, The University of Newcastle, Newcastle, NSW, Australia.
Hunter New England Population Health, Hunter New England Area Health Service, Newcastle, NSW, Australia.
Int J Behav Nutr Phys Act. 2021 Jan 22;18(1):16. doi: 10.1186/s12966-021-01080-4.
The 'scale-up' of effective physical activity interventions is required if they are to yield improvements in population health. The purpose of this study was to systematically review the effectiveness of community-based physical activity interventions that have been scaled-up. We also sought to explore differences in the effect size of these interventions compared with prior evaluations of their efficacy in more controlled contexts, and describe adaptations that were made to interventions as part of the scale-up process.
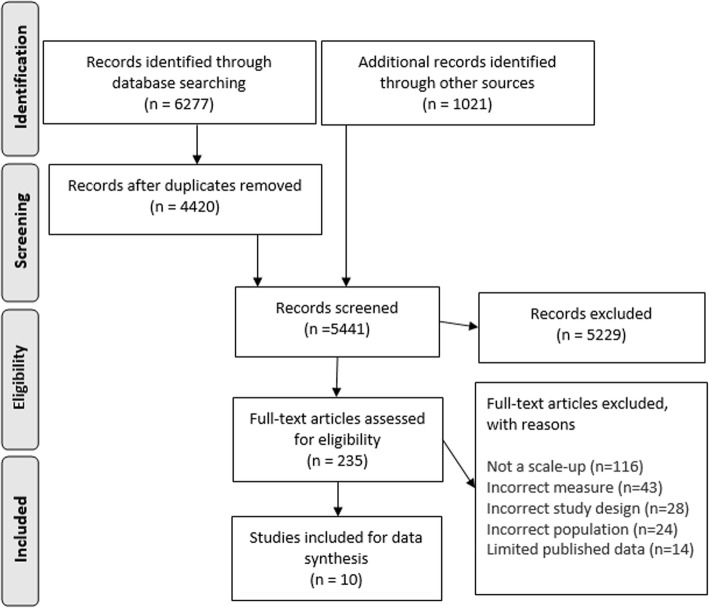
We performed a search of empirical research using six electronic databases, hand searched reference lists and contacted field experts. An intervention was considered 'scaled-up' if it had been intentionally delivered on a larger scale (to a greater number of participants, new populations, and/or by means of different delivery systems) than a preceding randomised control trial ('pre-scale') in which a significant intervention effect (p < 0.05) was reported on any measure of physical activity. Effect size differences between pre-scale and scaled up interventions were quantified ([the effect size reported in the scaled-up study / the effect size reported in the pre-scale-up efficacy trial] × 100) to explore any scale-up 'penalties' in intervention effects.
We identified 10 eligible studies. Six scaled-up interventions appeared to achieve significant improvement on at least one measure of physical activity. Six studies included measures of physical activity that were common between pre-scale and scaled-up trials enabling the calculation of an effect size difference (and potential scale-up penalty). Differences in effect size ranged from 132 to 25% (median = 58.8%), suggesting that most scaled-up interventions typically achieve less than 60% of their pre-scale effect size. A variety of adaptations were made for scale-up - the most common being mode of delivery.
The majority of interventions remained effective when delivered at-scale however their effects were markedly lower than reported in pre-scale trials. Adaptations of interventions were common and may have impacted on the effectiveness of interventions delivered at scale. These outcomes provide valuable insight for researchers and public health practitioners interested in the design and scale-up of physical activity interventions, and contribute to the growing evidence base for delivering health promotion interventions at-scale.
PROSPERO CRD42020144842 .
如果要提高人口健康水平,就需要对有效的身体活动干预措施进行“扩大规模”。本研究的目的是系统地审查已扩大规模的基于社区的身体活动干预措施的有效性。我们还试图探讨这些干预措施的效果大小与在更受控环境中对其疗效进行的先前评估之间的差异,并描述作为扩大规模过程的一部分对干预措施进行的调整。
我们使用六个电子数据库进行了实证研究搜索,对手头的参考文献进行了搜索,并联系了领域专家。如果干预措施是有意在更大规模上(对更多参与者、新人群和/或通过不同的交付系统)进行的,并且在先前的随机对照试验(“预规模”)中报告了任何身体活动测量的显著干预效果(p<0.05),则认为该干预措施是“扩大规模”。通过量化([扩大规模研究中报告的效果大小/预规模有效性试验中报告的效果大小]×100)干预措施效果之间的差异,来探索任何规模扩大的“惩罚”。
我们确定了 10 项符合条件的研究。六项扩大规模的干预措施似乎在至少一项身体活动测量上取得了显著改善。六项研究包括了预规模和扩大规模试验之间共有的身体活动测量,这使得能够计算效果大小差异(和潜在的扩大规模惩罚)。效果大小的差异范围从 132%到 25%(中位数=58.8%),这表明大多数扩大规模的干预措施通常只能达到其预规模效果大小的 60%以下。为了扩大规模,进行了各种调整-最常见的是交付方式。
当以规模化的方式提供时,大多数干预措施仍然有效,但它们的效果明显低于预规模试验中的报告。干预措施的调整很常见,可能会影响在规模上实施的干预措施的有效性。这些结果为对身体活动干预措施的设计和扩大规模感兴趣的研究人员和公共卫生从业人员提供了有价值的见解,并为在大规模上提供健康促进干预措施提供了不断增长的证据基础。
PROSPERO CRD42020144842。