Dukan Ruben, Amsallem Lior, Silvera Jonathan, Masmejean Emmanuel H
Department of Orthopaedic, Hand, Upper Limb and Peripheral Nerve Surgery Service, Georges-Pompidou European Hospital, 20, rue Leblanc 75015 Paris, France.
Department of Radiology, IMPC Bachaumont 6 rue Bachaumont 75002.
J Orthop Case Rep. 2020 Sep;10(6):44-48. doi: 10.13107/jocr.2020.v10.i06.1870.
Calcific tendinopathy of the pectoralis major at its humeral insertion is extremely rare. Few cases have been reported in the literature. We reported a unique case of calcification of the pectoralis major insertion site and conducted a review of the existing literature to propose standardized management.
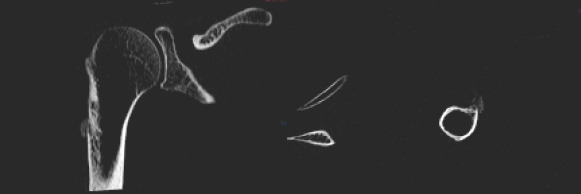
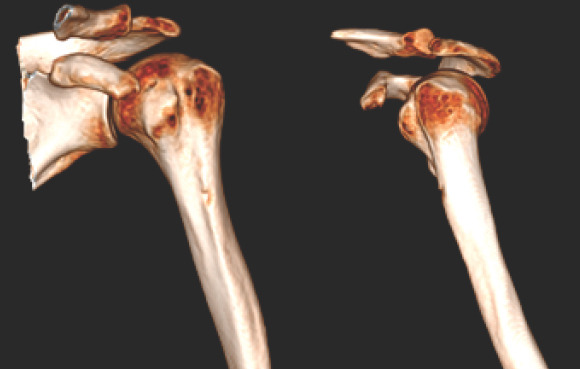
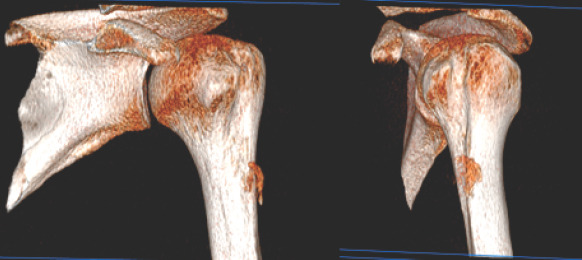
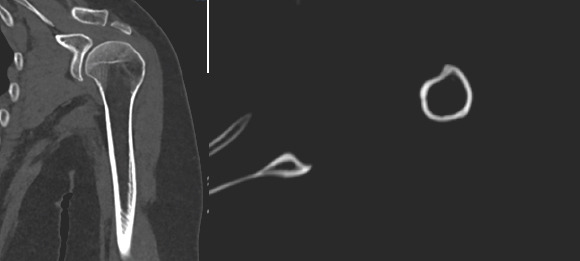
We reported a case of a 63-year-old lady, right-handed, non-smoker, homemaker without any history of trauma or symptoms suggestive of para-neoplasia syndrome. For 1 month, the patient presented severe, disabling pain of the left shoulder which occurred spontaneously, usually in the morning and after effort. The patient had painful passive terminal adduction and internal rotation. There was no neurovascular deficiency. Magnetic resonance imaging and computed tomography (CT) scan helped diagnose the calcific tendinopathy at the pectoralis major humeral insertion. Non-surgical management was performed, combining physiotherapy and painkillers. Two months' control, CT scan reported complete calcification resorption. The biologic assessment revealed hyperparathyroidism.
This rare and atypical localization can mislead the surgeon. A biological assessment to research a systemic etiology is mandatory and standardized. A biopsy is not required, radiological examinations are sufficient. Surgical treatment may be proposed in specific cases to shorten the necessary rehabilitation time.
胸大肌肱骨附着处的钙化性肌腱病极为罕见。文献中报道的病例很少。我们报告了一例胸大肌附着点钙化的独特病例,并对现有文献进行了综述,以提出标准化的治疗方案。
我们报告了一例63岁的女性患者,右利手,不吸烟,家庭主妇,无任何创伤史或副肿瘤综合征的症状提示。1个月来,患者出现左肩严重的、致残性疼痛,疼痛通常在早晨和用力后自发出现。患者被动终末内收和内旋时疼痛。无神经血管功能缺损。磁共振成像和计算机断层扫描(CT)有助于诊断胸大肌肱骨附着处的钙化性肌腱病。采取了非手术治疗,结合物理治疗和止痛药。经过两个月的观察,CT扫描显示钙化完全吸收。生物学评估显示甲状旁腺功能亢进。
这种罕见且非典型的定位可能会误导外科医生。必须进行生物学评估以寻找全身性病因且评估应标准化。无需进行活检,放射学检查就足够了。在特定情况下可考虑手术治疗,以缩短必要的康复时间。