Truong Michael, Rane Madhura S, Govere Sabina, Galagan Sean R, Moosa Mahomed-Yunus, Stoep Ann Vander, Celum Connie, Drain Paul K
Department of Epidemiology, School of Public Health, University of Washington, 1959 Pacific St, Seattle, WA 98195, United States.
AIDS Healthcare Foundation, Durban, South Africa.
EClinicalMedicine. 2021 Jan 7;31:100621. doi: 10.1016/j.eclinm.2020.100621. eCollection 2021 Jan.
Since mental health may influence HIV care among people living with HIV (PLHIV), we sought to evaluate the impact of anxiety and depression on ART initiation and HIV-related outcomes.
We conducted a prospective cohort study of PLHIV in the Umlazi Township of KwaZulu-Natal, South Africa. We measured depression using the Patient Health Questionnaire (PHQ-9) and anxiety using the Generalized Anxiety Disorder (GAD-7) scale, both of which have been validated in sub-Saharan Africa, among all patients prior to receiving a positive HIV test. We then followed those who tested HIV+ for 12 months to determine their time to ART initiation, missing clinic visits or refills, retention in care, hospitalization, and death. We used logistic regression models, adjusted for socio-demographic characteristics such as age and sex, to examine the effects of baseline measures of depression and anxiety on ART initiation and HIV treatment outcomes.
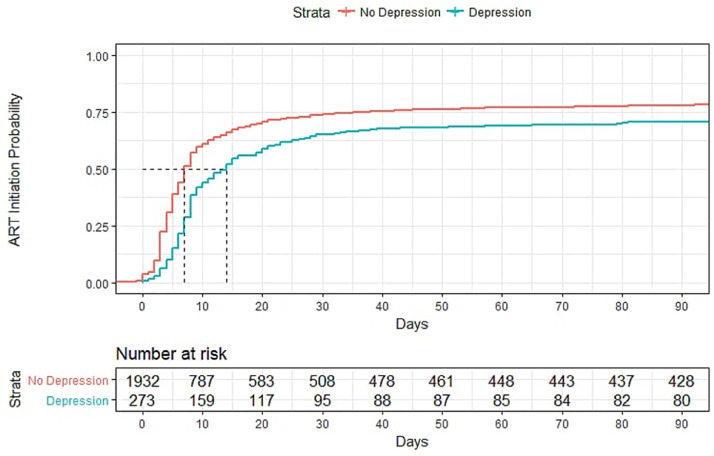
Among 2,319 adult PLHIV, mean age was 33 years (SD=9.3 years), 57% were female, and baseline median CD4 count was 317 cells/mm (IQR=175-491 cells/mm). In univariate analyses, depression was associated with slower rates of ART initiation. In adjusted models, PLHIV with depression had lower odds of initiating ART within 90 days of HIV testing (aOR=0.60, 95% CI=0.46, 0.79, <0.01), and lower odds of being retained in care (aOR=0.77, 95% CI=0.60, 0.99, = 0.04). By the end of the 12-month study period, odds of ART initiation among PLHIV with depression were higher than the first 90 days but still significantly lower compared to those without depression (aOR=0.72, 95% CI=0.52, 0.99, = 0.04). Among PLHIV who initiated ART, depression was associated with a lower odds of missing clinic visits (aOR=0.54, 95% CI= 0.40, 0.73, <0.01). Anxiety was strongly correlated with depression ( = 0.77, <0.01) and had similar effects on HIV-related outcomes.
The presence of depression is a significant barrier to ART initiation and retention in care among adult PLHIV in South Africa. Mental health screenings around the time of HIV testing may help improve linkage and HIV-related outcomes.
This work was supported by the Infectious Disease Society of America Education & Research Foundation and National Foundation for Infectious Diseases (PKD); Massachusetts General Hospital Executive Committee on Research (PKD); the Harvard University Center for AIDS Research [AI060354] (PKD); and the National Institute of Allergy and Infectious Diseases [AI108293, AI143351] (PKD). The content is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health or other funding agencies.
由于心理健康可能会影响艾滋病病毒感染者(PLHIV)的艾滋病护理情况,我们试图评估焦虑和抑郁对开始抗逆转录病毒治疗(ART)及与艾滋病相关结局的影响。
我们在南非夸祖鲁 - 纳塔尔省的乌姆拉齐镇对艾滋病病毒感染者进行了一项前瞻性队列研究。在所有患者进行艾滋病病毒检测呈阳性之前,我们使用患者健康问卷(PHQ - 9)测量抑郁情况,使用广泛性焦虑障碍(GAD - 7)量表测量焦虑情况,这两种量表在撒哈拉以南非洲地区均已得到验证。然后,我们对那些检测出艾滋病病毒呈阳性的患者进行了12个月的随访,以确定他们开始接受抗逆转录病毒治疗的时间、错过门诊就诊或药物 refill 的情况、持续接受治疗的情况、住院情况以及死亡情况。我们使用逻辑回归模型,并对年龄和性别等社会人口学特征进行了调整,以研究抑郁和焦虑的基线测量值对开始抗逆转录病毒治疗及艾滋病治疗结局的影响。
在2319名成年艾滋病病毒感染者中,平均年龄为33岁(标准差 = 9.3岁),57%为女性,基线CD4细胞计数中位数为317个/立方毫米(四分位间距 = 175 - 491个/立方毫米)。在单变量分析中,抑郁与开始抗逆转录病毒治疗的速度较慢有关。在调整后的模型中,患有抑郁症的艾滋病病毒感染者在艾滋病病毒检测后90天内开始接受抗逆转录病毒治疗的几率较低(调整后的比值比[aOR]=0.60,95%置信区间[CI]=0.46,0.79,P<0.01),持续接受治疗的几率也较低(aOR = 0.77,95% CI = 0.60,0.99,P = 0.04)。到12个月研究期结束时,患有抑郁症的艾滋病病毒感染者开始接受抗逆转录病毒治疗的几率高于最初的90天,但与没有抑郁症的感染者相比仍显著较低(aOR = 0.72,95% CI = 0.52,0.99,P = 0.04)。在开始接受抗逆转录病毒治疗的艾滋病病毒感染者中,抑郁与错过门诊就诊的几率较低有关(aOR = 0.54,95% CI = 0.40,0.73,P<0.01)。焦虑与抑郁密切相关(相关系数 = 0.77,P<0.01),并且对与艾滋病相关的结局有类似影响。
抑郁症的存在是南非成年艾滋病病毒感染者开始接受抗逆转录病毒治疗及持续接受治疗的一个重大障碍。在艾滋病病毒检测前后进行心理健康筛查可能有助于改善治疗衔接及与艾滋病相关的结局。
这项工作得到了美国传染病学会教育与研究基金会和国家传染病基金会(PKD);麻省总医院研究执行委员会(PKD);哈佛大学艾滋病研究中心[AI060354](PKD);以及国家过敏和传染病研究所[AI108293,AI143351](PKD)的支持。内容完全由作者负责,并不代表美国国立卫生研究院或其他资助机构的官方观点。