Department of Critical Care Medicine, Shanghai Children's Hospital, Shanghai Jiao Tong University, Shanghai, 200062, China.
Institute of Pediatric Critical Care, Shanghai Jiao Tong University, No.355 Luding Road, Putuo District, Shanghai, 200062, China.
BMC Pulm Med. 2021 Jan 25;21(1):40. doi: 10.1186/s12890-021-01394-w.
Lung ultrasound score is a potential method for determining pulmonary edema in acute respiratory distress syndrome (ARDS). Continuous renal replacement therapy (CRRT) has become the preferred modality to manage fluid overload during ARDS. The aim of this study was to evaluate the value of lung ultrasound (LUS) score on assessing the effects of CRRT on pulmonary edema and pulmonary function in pediatric ARDS.
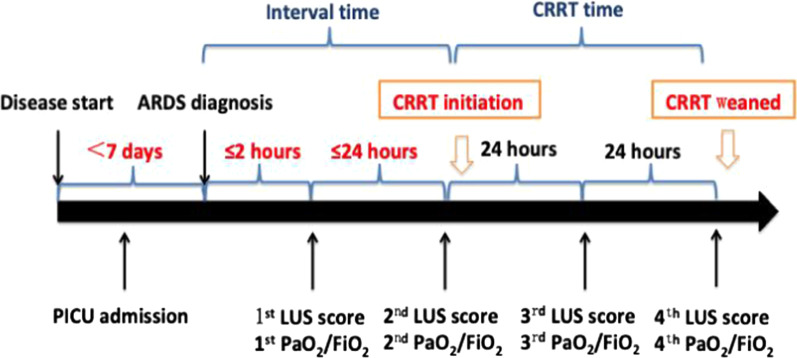
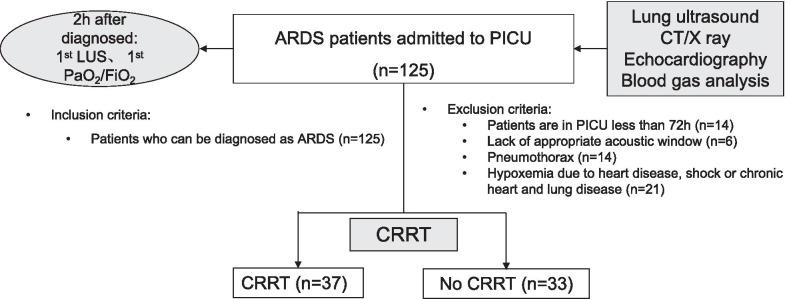
We conducted a prospective cohort study in 70 children with moderate to severe ARDS in a tertiary university pediatric intensive care unit from January 2016 to December 2019. 37 patients received CRRT (CRRT group) and 33 patients treated by conventional therapy (Non-CRRT group). LUS score was measured within 2 h identified ARDS as the value of 1st, and the following three days as the 2nd, 3rd, and 4th. We used Spearman correlation analysis to develop the relationship between LUS score and parameters related to respiratory dynamics, clinical outcomes as well as daily fluid balance during the first four days after ARDS diagnosed.
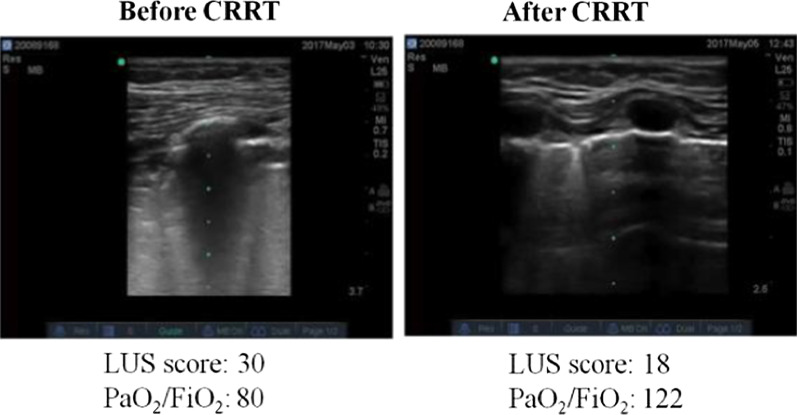
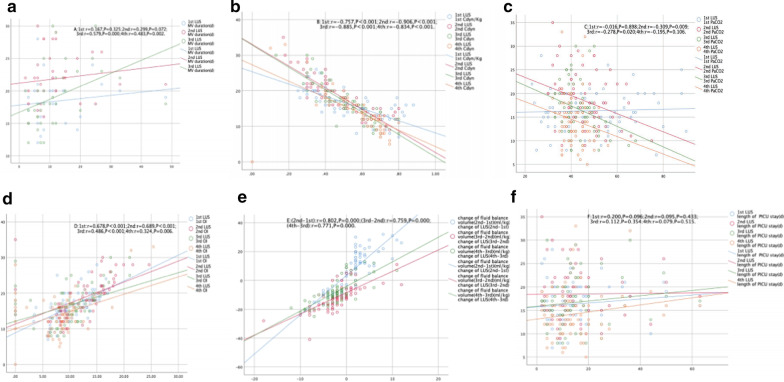
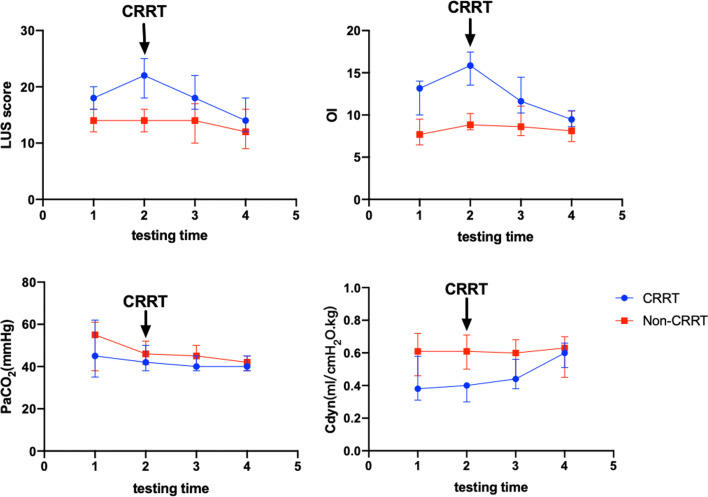
The 1st LUS score in CRRT group were significantly higher than Non-CRRT group (P < 0.001), but the LUS score decreased gradually following CRRT (P < 0.001). LUS score was significantly correlated with Cdyn (dynamic lung compliance) (1st: r = - 0.757, 2nd: r = - 0.906, 3rd: r = - 0.885, 4th: r = - 0.834), OI (oxygenation index) (1st: r = 0.678, 2nd: r = 0.689, 3rd: r = 0.486, 4th: r = 0.324) based on 1st to 4th values (all P < 0.05). Only values of the 3rd and 4th LUS score after ARDS diagnosed were correlated with duration of mechanical ventilation [1st: r = 0.167, P = 0.325; 2nd: r = 0.299, P = 0.072; 3rd: r = 0.579, P < 0.001; 4th: r = 0.483, P = 0.002]. LUS score decreased from 22 (18-25) to 15 (13-18) and OI decreased from 15.92 (14.07-17.73) to 9.49 (8.70-10.58) after CRRT for four days (both P < 0.001).
LUS score is significantly correlated with lung function parameters in pediatric ARDS. The improvement of pulmonary edema in patient with ARDS received CRRT can be assessed by the LUS score. Trial registration CCTR, ChiCTR-ONC-16009698. Registered 1 November 2016, prospectively registered, http://www.chictr.org.cn/edit.aspx?pid=16535&htm=4 . This study adheres to CONSORT guidelines.
肺部超声评分是一种确定急性呼吸窘迫综合征(ARDS)肺部水肿的潜在方法。连续性肾脏替代疗法(CRRT)已成为治疗 ARDS 中液体超负荷的首选方式。本研究旨在评估肺部超声(LUS)评分在评估 CRRT 对儿科 ARDS 肺部水肿和肺功能的影响。
我们在 2016 年 1 月至 2019 年 12 月期间,对一家三级大学儿科重症监护病房的 70 名中度至重度 ARDS 患儿进行了前瞻性队列研究。37 名患者接受了 CRRT(CRRT 组),33 名患者接受了常规治疗(非-CRRT 组)。在 ARDS 确诊后的 2 小时内,通过 LUS 评分测量值为 1 分,随后的三天分别为 2 分、3 分和 4 分。我们使用 Spearman 相关分析来建立 LUS 评分与呼吸动力学参数、临床结果以及 ARDS 确诊后前四天每日液体平衡之间的关系。
CRRT 组的第 1 次 LUS 评分明显高于非-CRRT 组(P<0.001),但随着 CRRT 的进行,LUS 评分逐渐下降(P<0.001)。LUS 评分与 Cdyn(动态肺顺应性)(第 1 次:r=−0.757,第 2 次:r=−0.906,第 3 次:r=−0.885,第 4 次:r=−0.834)和 OI(氧合指数)(第 1 次:r=0.678,第 2 次:r=0.689,第 3 次:r=0.486,第 4 次:r=0.324)显著相关,所有相关系数均在第 1 次到第 4 次测量值中均有统计学意义(均 P<0.05)。只有 ARDS 确诊后的第 3 次和第 4 次 LUS 评分与机械通气时间相关[第 1 次:r=0.167,P=0.325;第 2 次:r=0.299,P=0.072;第 3 次:r=0.579,P<0.001;第 4 次:r=0.483,P=0.002]。CRRT 治疗 4 天后,LUS 评分从 22(18-25)降至 15(13-18),OI 从 15.92(14.07-17.73)降至 9.49(8.70-10.58)(均 P<0.001)。
LUS 评分与儿科 ARDS 的肺功能参数显著相关。接受 CRRT 的 ARDS 患者肺部水肿的改善可通过 LUS 评分来评估。临床试验注册 CCTR,ChiCTR-ONC-16009698。2016 年 11 月 1 日注册,前瞻性注册,http://www.chictr.org.cn/edit.aspx?pid=16535&htm=4。本研究符合 CONSORT 指南。