Bellasi Antonio, Di Lullo Luca, Russo Domenico, Ciarcia Roberto, Magnocavallo Michele, Lavalle Carlo, Ratti Carlo, Fusaro Maria, Cozzolino Mario, Di Iorio Biagio Raffaele
Department of Research, Innovation and Brand Reputation, ASST Papa Giovanni XXIII, 24127 Bergamo, Italy.
Department of Nephrology and Dialysis, Ospedale Parodi, Delfino, 00034 Colleferro, Italy.
J Clin Med. 2021 Jan 20;10(3):376. doi: 10.3390/jcm10030376.
Vascular calcification (VC) is a marker of cardiovascular (CV) disease and various methods allow for presence and extension assessment in different arterial districts. Nevertheless, it is currently unclear which one of these methods for VC evaluation best predict outcome and if this piece of information adds to the predictive value of traditional CV risk factors in patients receiving hemodialysis (HD).
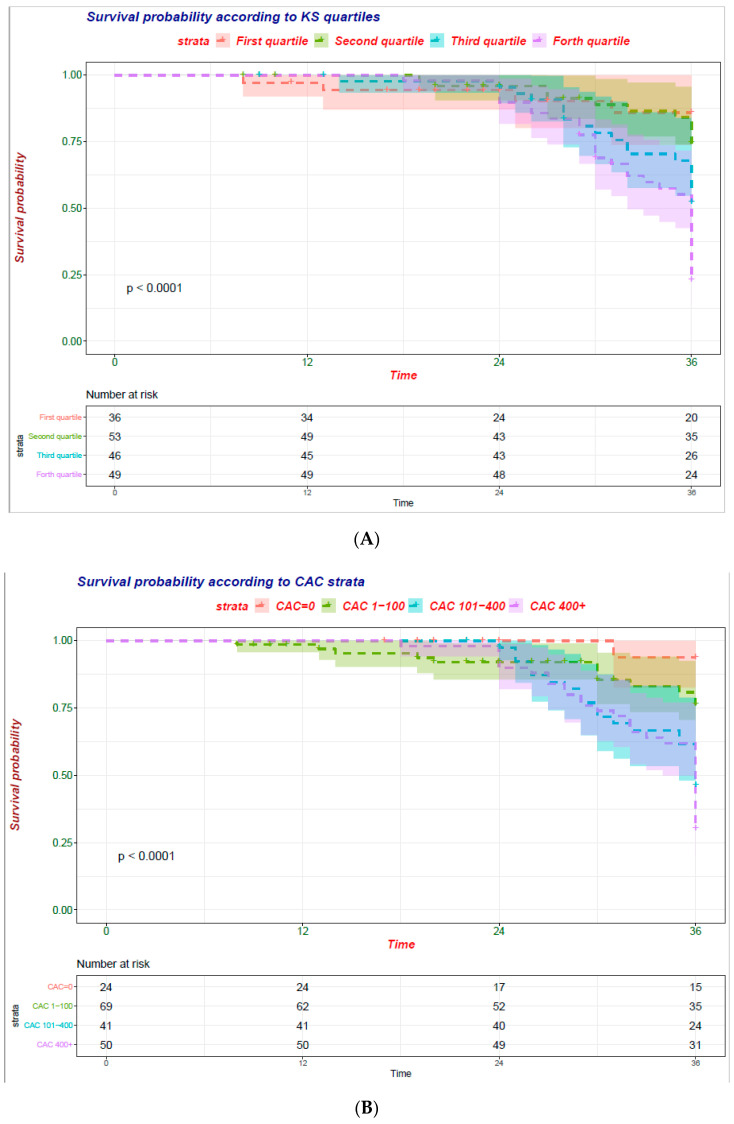
data of 184 of the 466 patients followed in the Independent study (NCT00710788) were post hoc examined to assess the association three concurrent measures of vascular calcification and all-cause survival. Specifically, coronary artery calcification (CAC) was determined by the Agatston and the volume score while abdominal aorta calcification was determined by plain X-ray of the lumbar spine (Kauppila score (KS)). Survival and regression models as well as metrics of risk recalculation were used to test the association of VC and outcome beyond the Framingham risk score.
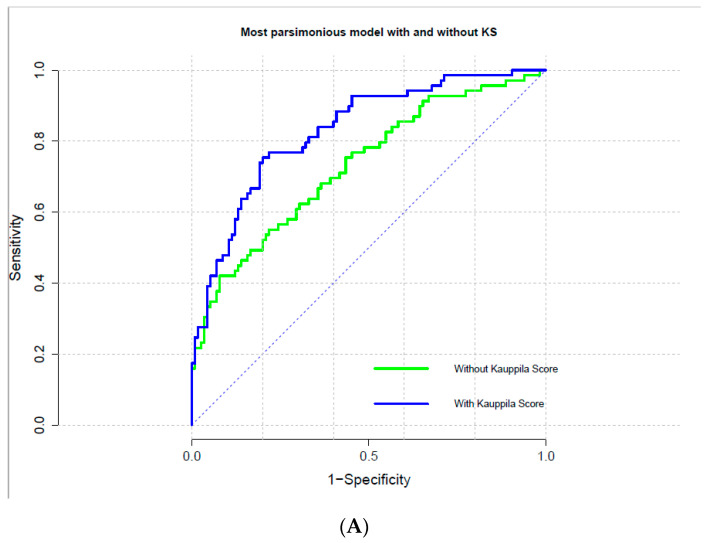
Middle-age (62.6(15.8) years) men (51%) and women (49%) starting HD were analyzed. Over 36 (median 36; interquartile range: 8-36) months of follow-up 69 patients expired. Each measure of VC (CAC or KS) predicted all-cause mortality independently factors commonly associated with all-cause survival ( < 0.001). Far more importantly, each measurement of VC significantly improved risk prediction and patient reclassification ( < 0.001) beyond traditional cardiovascular risk factors.
Overall, presence and extension of VC, irrespective of the arterial site, predict risk of all-cause of death in patients starting hemodialysis. Of note, both CAC and KS increase risk stratification beyond traditional CV risk factors. However, future efforts are needed to assess whether a risk-based approach encompassing VC screening to guide HD patient management improves survival.
血管钙化(VC)是心血管疾病(CV)的一个标志物,多种方法可用于评估不同动脉区域的血管钙化情况及其范围。然而,目前尚不清楚这些评估VC的方法中哪一种最能预测预后,以及这一信息是否能增加接受血液透析(HD)患者传统CV危险因素的预测价值。
对独立研究(NCT00710788)中随访的466例患者中的184例数据进行事后分析,以评估三种同时进行的血管钙化测量方法与全因生存的相关性。具体而言,冠状动脉钙化(CAC)通过阿加斯顿评分和体积评分来确定,而腹主动脉钙化则通过腰椎平片(考皮拉评分(KS))来确定。使用生存和回归模型以及风险重新计算指标来测试VC与超出弗雷明汉姆风险评分的预后之间的关联。
分析了开始进行HD的中年(62.6(15.8)岁)男性(51%)和女性(49%)。在超过36(中位数36;四分位间距:8 - 36)个月的随访期内,69例患者死亡。每种VC测量方法(CAC或KS)均独立预测全因死亡率,且与全因生存的常见相关因素有关(P < 0.001)。更重要的是,与传统心血管危险因素相比,每种VC测量方法都显著改善了风险预测和患者重新分类(P < 0.001)。
总体而言,无论动脉部位如何,VC的存在和范围均可预测开始血液透析患者的全因死亡风险。值得注意的是,CAC和KS均能在传统CV危险因素之外增加风险分层。然而,未来需要努力评估基于风险的方法(包括VC筛查)以指导HD患者管理是否能改善生存情况。