Division of Transplantation Surgery, Department of Clinical Science, Intervention and Technology, Karolinska University Hospital, Karolinska Institutet, Stockholm, Sweden.
Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden.
J Intern Med. 2022 Jun;291(6):813-823. doi: 10.1111/joim.13459. Epub 2022 Feb 11.
Progression of vascular calcification causes cardiovascular disease, which is the most common cause of death in chronic kidney failure and after kidney transplantation (KT). The prognostic impact of the extent of medial vascular calcification at KT is unknown.
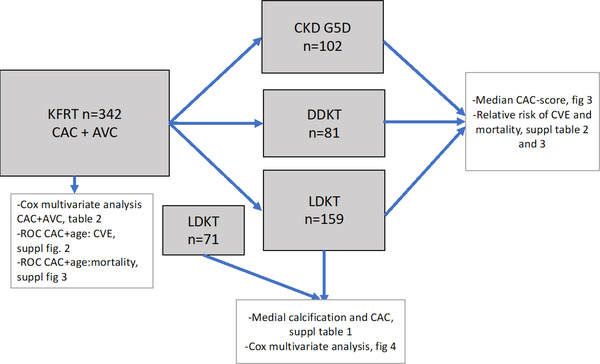
In this prospective cohort study, we investigated the impact of medial calcification compared to a mix of intimal and medial calcification represented by coronary artery calcification (CAC score) and aortic valve calcification in 342 patients starting on kidney failure replacement therapy. The primary outcomes were cardiovascular events (CVE) and death. The median follow-up time was 6.4 years (interquartile range 3.7-9.6 years). Exposure was CAC score and arteria epigastrica medial calcification scored as none, mild, moderate, or severe by a pathologist at time of KT (n = 200). We divided the patients according to kidney failure replacement therapy during follow-up, that is, living donor KT, deceased donor KT, or dialysis.
Moderate to severe medial calcification in the arteria epigastrica was associated with higher mortality (p = 0.001), and the hazard ratio for CVE was 3.1 (95% confidence interval [CI] 1.12-9.02, p < 0.05) compared to no or mild medial calcification. The hazard ratio for 10-year mortality in the dialysis group was 33.6 (95% CI, 10.0-113.0, p < 0.001) compared to living donor recipients, independent of Framingham risk score and prevalent CAC.
Scoring of medial calcification in the arteria epigastrica identified living donor recipients as having 3.1 times higher risk of CVE, independent of traditional risk factors. The medial calcification score could be a reliable method to identify patients with high and low risk of CVE and mortality following KT.
血管钙化的进展导致心血管疾病,这是慢性肾衰竭和肾移植(KT)后最常见的死亡原因。KT 时中层血管钙化程度对预后的影响尚不清楚。
在这项前瞻性队列研究中,我们研究了与冠状动脉钙化(CAC 评分)和主动脉瓣钙化所代表的内膜和中层混合钙化相比,中层钙化对开始肾衰竭替代治疗的 342 例患者的影响。主要结局为心血管事件(CVE)和死亡。中位随访时间为 6.4 年(四分位间距 3.7-9.6 年)。暴露为 CAC 评分和在 KT 时由病理学家评估的腹主动脉中层钙化(n=200),分为无、轻度、中度或重度。我们根据随访期间的肾衰竭替代治疗将患者分为活体供肾 KT、已故供肾 KT 或透析。
腹主动脉中度至重度中层钙化与死亡率升高相关(p=0.001),与无或轻度中层钙化相比,CVE 的危险比为 3.1(95%置信区间[CI]1.12-9.02,p<0.05)。与活体供体受者相比,透析组的 10 年死亡率危险比为 33.6(95%CI,10.0-113.0,p<0.001),独立于弗雷明汉风险评分和 CAC 患病率。
腹主动脉中层钙化评分确定了活体供体受者发生 CVE 的风险高 3.1 倍,独立于传统危险因素。中层钙化评分可能是一种可靠的方法,可用于识别 KT 后 CVE 和死亡率高风险和低风险的患者。