Department of Cardiology, The Rayne Institute, St Thomas' Hospital, British Heart Foundation Centre of Research Excellence, School of Cardiovascular Medicine and Sciences, King's College London, UK.
Mediators Inflamm. 2021 Jan 14;2021:8874339. doi: 10.1155/2021/8874339. eCollection 2021.
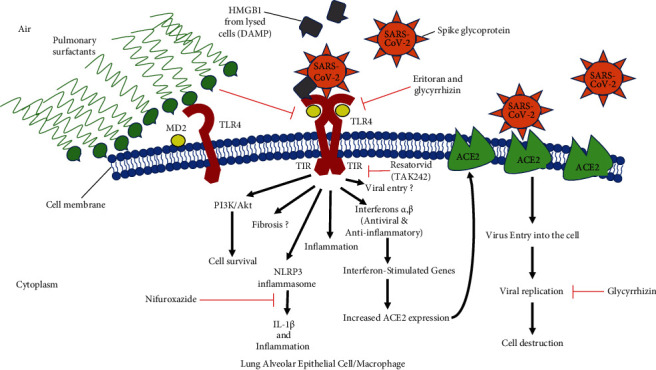
Causes of mortality from COVID-19 include respiratory failure, heart failure, and sepsis/multiorgan failure. TLR4 is an innate immune receptor on the cell surface that recognizes pathogen-associated molecular patterns (PAMPs) including viral proteins and triggers the production of type I interferons and proinflammatory cytokines to combat infection. It is expressed on both immune cells and tissue-resident cells. ACE2, the reported entry receptor for SARS-CoV-2, is only present on ~1-2% of the cells in the lungs or has a low pulmonary expression, and recently, the spike protein has been proposed to have the strongest protein-protein interaction with TLR4. Here, we review and connect evidence for SARS-CoV-1 and SARS-CoV-2 having direct and indirect binding to TLR4, together with other viral precedents, which when combined shed light on the COVID-19 pathophysiological puzzle. We propose a model in which the SARS-CoV-2 spike glycoprotein binds TLR4 and activates TLR4 signalling to increase cell surface expression of ACE2 facilitating entry. SARS-CoV-2 also destroys the type II alveolar cells that secrete pulmonary surfactants, which normally decrease the air/tissue surface tension and block TLR4 in the lungs thus promoting ARDS and inflammation. Furthermore, SARS-CoV-2-induced myocarditis and multiple-organ injury may be due to TLR4 activation, aberrant TLR4 signalling, and hyperinflammation in COVID-19 patients. Therefore, TLR4 contributes significantly to the pathogenesis of SARS-CoV-2, and its overactivation causes a prolonged or excessive innate immune response. TLR4 appears to be a promising therapeutic target in COVID-19, and since TLR4 antagonists have been previously trialled in sepsis and in other antiviral contexts, we propose the clinical trial testing of TLR4 antagonists in the treatment of severe COVID-19. Also, ongoing clinical trials of pulmonary surfactants in COVID-19 hold promise since they also block TLR4.
COVID-19 的死亡原因包括呼吸衰竭、心力衰竭和败血症/多器官衰竭。TLR4 是细胞表面的先天免疫受体,可识别病原体相关分子模式(PAMPs),包括病毒蛋白,并触发 I 型干扰素和促炎细胞因子的产生,以抵抗感染。它在免疫细胞和组织驻留细胞上均有表达。ACE2 是报告的 SARS-CoV-2 进入受体,仅存在于肺部约 1-2%的细胞上或肺表达水平较低,最近有人提出,刺突蛋白与 TLR4 的蛋白-蛋白相互作用最强。在这里,我们回顾并连接了 SARS-CoV-1 和 SARS-CoV-2 与 TLR4 的直接和间接结合的证据,以及其他病毒的先例,这些证据结合起来阐明了 COVID-19 的病理生理学难题。我们提出了一个模型,其中 SARS-CoV-2 刺突糖蛋白与 TLR4 结合并激活 TLR4 信号通路,增加 ACE2 的细胞表面表达,从而促进进入。SARS-CoV-2 还破坏了分泌肺表面活性剂的 II 型肺泡细胞,肺表面活性剂通常会降低空气/组织表面张力并阻断肺部的 TLR4,从而促进 ARDS 和炎症。此外,SARS-CoV-2 诱导的心肌炎和多器官损伤可能是由于 TLR4 的激活、异常的 TLR4 信号和 COVID-19 患者的过度炎症。因此,TLR4 对 SARS-CoV-2 的发病机制有重要贡献,其过度激活会导致持续或过度的先天免疫反应。TLR4 似乎是 COVID-19 的一个有前途的治疗靶点,并且由于 TLR4 拮抗剂以前已在败血症和其他抗病毒环境中进行了试验,因此我们建议在治疗严重 COVID-19 中测试 TLR4 拮抗剂的临床试验。此外,COVID-19 中肺表面活性剂的正在进行的临床试验也有希望,因为它们也能阻断 TLR4。