Ahmadipour Yahya, Rauschenbach Laurèl, Santos Alejandro, Darkwah Oppong Marvin, Lazaridis Lazaros, Quesada Carlos M, Junker Andreas, Pierscianek Daniela, Dammann Philipp, Wrede Karsten H, Scheffler Björn, Glas Martin, Stuschke Martin, Sure Ulrich, Jabbarli Ramazan
Department of Neurosurgery and Spine Surgery, University Hospital Essen, Essen, Germany.
German Cancer Consortium, Partner Site University Hospital Essen, Essen, Germany.
Neurooncol Adv. 2020 Nov 18;3(1):vdaa158. doi: 10.1093/noajnl/vdaa158. eCollection 2021 Jan-Dec.
Symptomatic epilepsy is a common symptom of glioblastoma, which may occur in different stages of disease. There are discrepant reports on association between early seizures and glioblastoma survival, even less is known about the background of these seizures. We aimed at analyzing the risk factors and clinical impact of perioperative seizures in glioblastoma.
All consecutive cases with de-novo glioblastoma treated at our institution between 01/2006 and 12/2018 were eligible for this study. Perioperative seizures were stratified into seizures at onset (SAO) and early postoperative seizures (EPS, ≤21days after surgery). Associations between patients characteristics and overall survival (OS) with SAO and EPS were addressed.
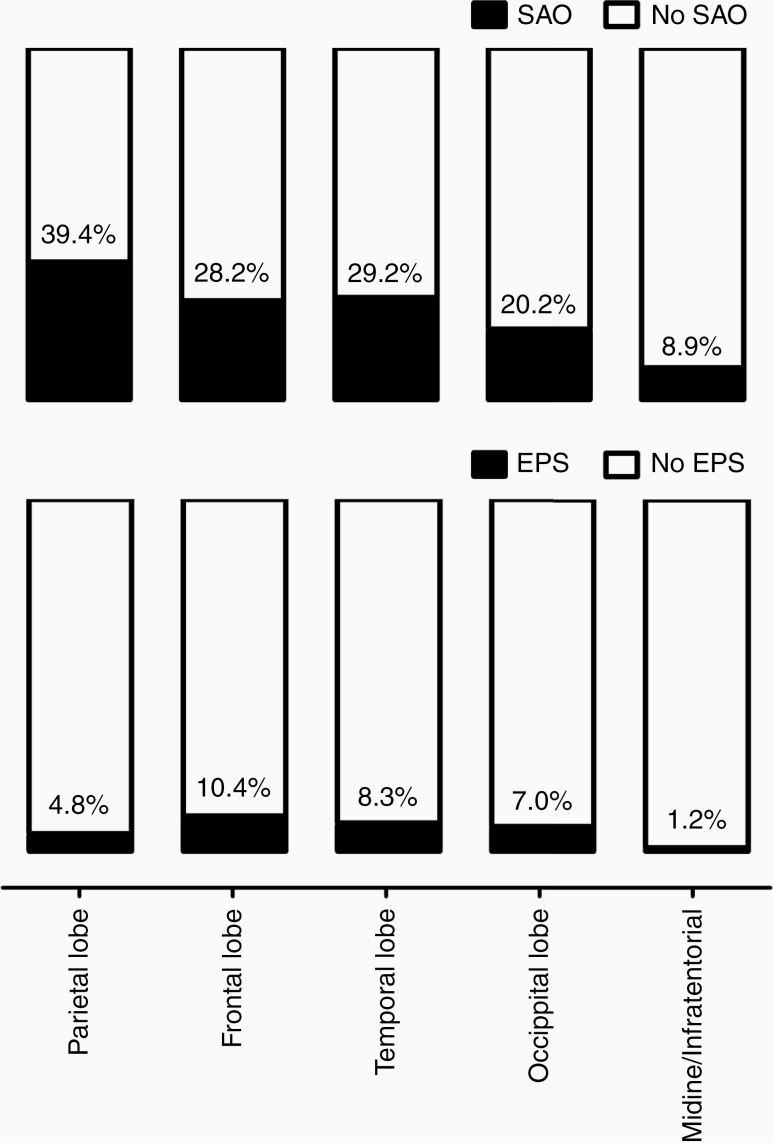
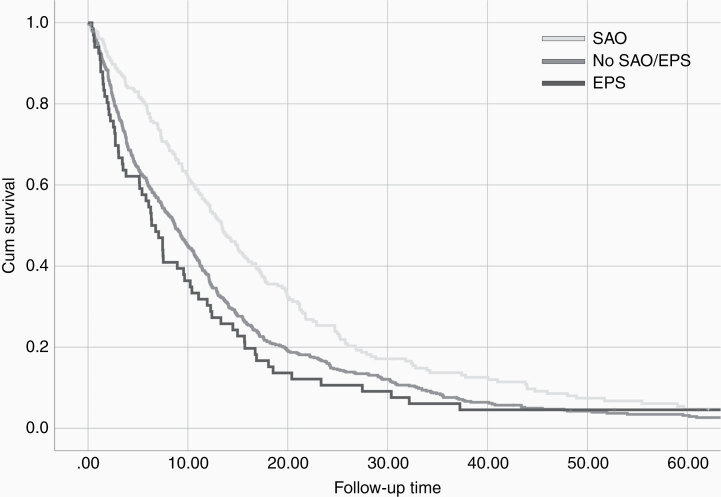
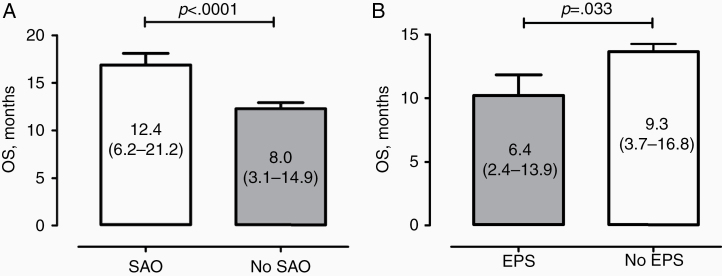
In the final cohort ( = 867), SAO and EPS occurred in 236 (27.2%) and 67 (7.7%) patients, respectively. SAO were independently predicted by younger age ( = .009), higher KPS score ( = .002), tumor location (parietal lobe, = .001), GFAP expression (≥35%, = .045), and serum chloride at admission (>102 mmol/L, = .004). In turn, EPS were independently associated with tumor location (frontal or temporal lobe, = .013) and pathologic laboratory values at admission (hemoglobin < 12 g/dL, [ = .044], CRP > 1.0 mg/dL [ = 0.036], and GGT > 55 U/L [ = 0.025]). Finally, SAO were associated with gross-total resection ( = .006) and longer OS ( = .030), whereas EPS were related to incomplete resection ( = .005) and poorer OS ( = .009).
In glioblastoma patients, SAO and EPS seem to have quite different triggers and contrary impact on treatment success and OS. The clinical characteristics of SAO and EPS patients might contribute to the observed survival differences.
症状性癫痫是胶质母细胞瘤的常见症状,可能发生在疾病的不同阶段。关于早期癫痫发作与胶质母细胞瘤生存期之间的关联,报道存在差异,而这些癫痫发作的背景情况则知之更少。我们旨在分析胶质母细胞瘤围手术期癫痫发作的危险因素及临床影响。
2006年1月至2018年12月期间在本机构接受治疗的所有初发性胶质母细胞瘤连续病例均符合本研究条件。围手术期癫痫发作分为发病时癫痫发作(SAO)和术后早期癫痫发作(EPS,术后≤21天)。探讨患者特征以及SAO和EPS与总生存期(OS)之间的关联。
在最终队列(n = 867)中,SAO和EPS分别发生在236例(27.2%)和67例(7.7%)患者中。SAO的独立预测因素为年龄较小(p = 0.009)、较高的KPS评分(p = 0.002)、肿瘤位置(顶叶,p = 0.001)、GFAP表达(≥35%,p = 0.045)以及入院时血清氯水平(>102 mmol/L,p = 0.004)。反过来,EPS与肿瘤位置(额叶或颞叶,p = 0.013)以及入院时的病理实验室值(血红蛋白<12 g/dL,[p = 0.044],CRP>1.0 mg/dL [p = 0.036],以及GGT>55 U/L [p = 0.025])独立相关。最后,SAO与大体全切除(p = 0.006)和较长的OS(p = 0.030)相关,而EPS与不完全切除(p = 0.005)和较差的OS(p = 0.009)相关。
在胶质母细胞瘤患者中,SAO和EPS似乎具有截然不同的触发因素,并且对治疗成功和OS有相反的影响。SAO和EPS患者的临床特征可能导致观察到的生存期差异。