Department of Orthopedics, Örebro University School of Medical Sciences and Örebro University Hospital, Örebro, Sweden.
Acta Orthop. 2021 Jun;92(3):264-268. doi: 10.1080/17453674.2021.1879505. Epub 2021 Jan 28.
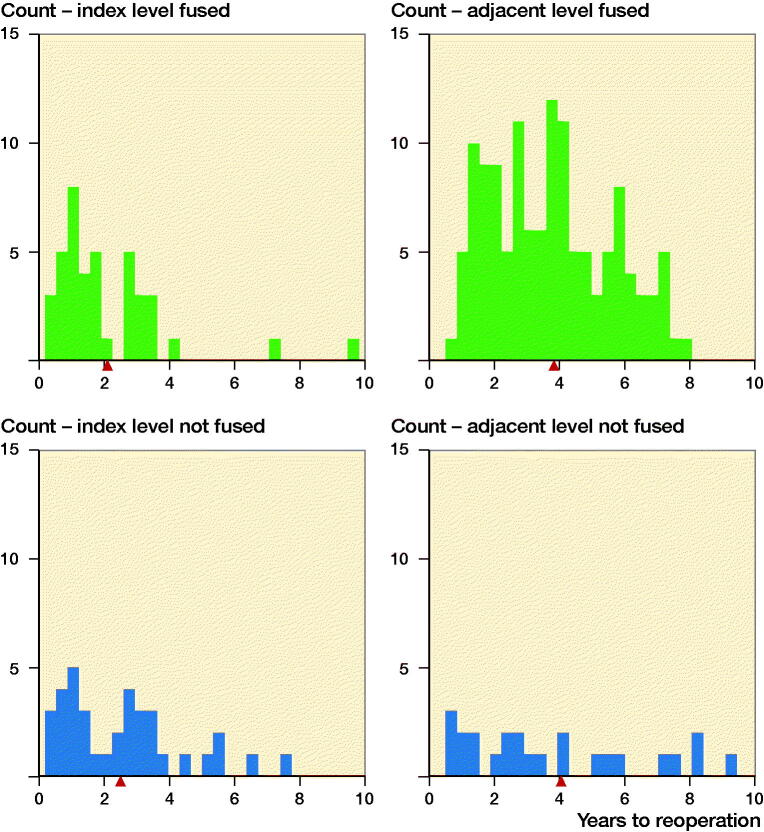
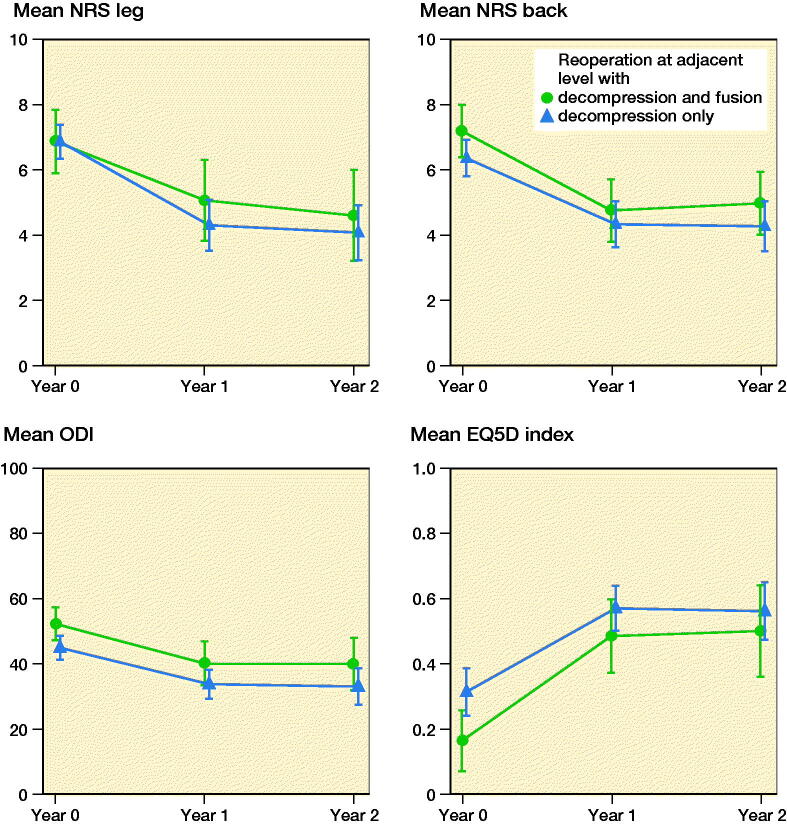
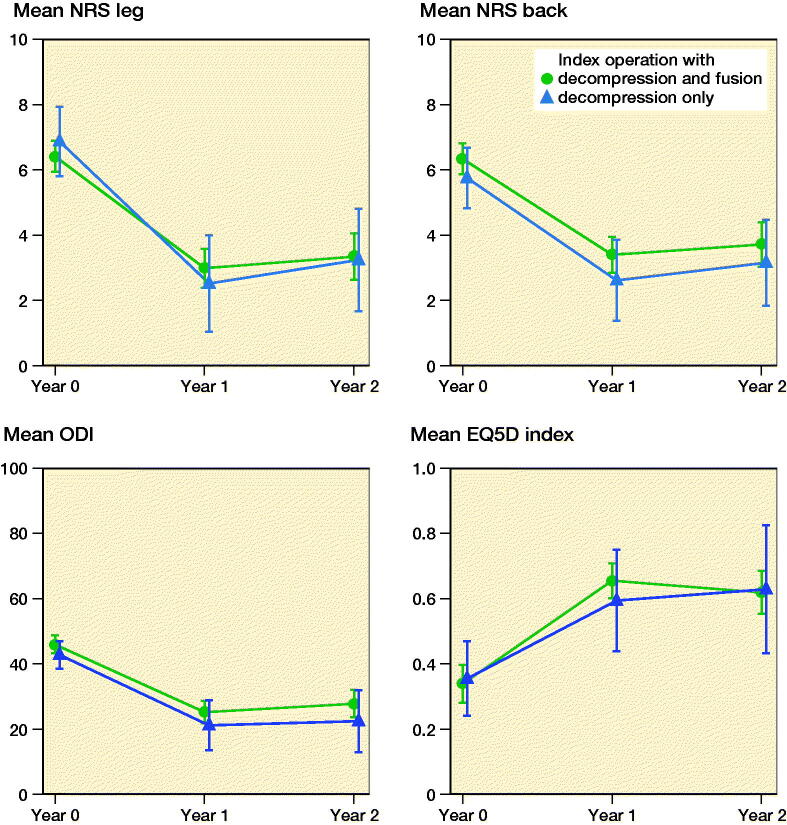
Background and purpose - There are different opinions on how to surgically address lumbar spinal stenosis with concomitant degenerative spondylolisthesis (DS). We investigated reoperation rates at the index and adjacent levels after L4-5 fusion surgery in a large cohort of unselected patients registered in Swespine, the national Swedish spine register.Patients and methods - 6,532 patients, who underwent surgery for L4-5 spinal stenosis with or without DS between 2007 and 2012, were followed up to 2017 to identify reoperations at the index and adjacent levels. The reoperation rates for decompression and fusion were compared with the reoperation rates for decompression only and for patients with or without DS. Patient-reported outcome data were collected preoperatively, and at 1 and 2 years after surgery and used to evaluate differences in outcome between index operations and reoperations.Results - For spinal stenosis with DS, the reoperation rate at the index level was 3.0% for decompression and fusion and 6.0% for decompression only. At the adjacent level, the corresponding numbers were 9.7% and 4.2% respectively. For spinal stenosis without DS, the reoperation rate at the index level was 3.7% for decompression and fusion and 6.2% after decompression only. At the adjacent level, the corresponding numbers were 8.1% and 3.8% respectively. For the reoperations at the adjacent level, there was no difference in patient-reported outcome between extended fusion or decompression only.Interpretation - Single-level lumbar fusion surgery is associated with an increased rate of reoperations at the adjacent level compared with decompression only. When reoperations at the index level are included there is no difference in reoperation rates between fusion and decompression only.
背景与目的-对于合并退行性腰椎滑脱(DS)的腰椎管狭窄症如何进行手术治疗,存在不同意见。我们在瑞典全国脊柱登记处(Swespine)的一项未经选择的大样本患者队列中研究了 L4-5 融合术后指数和相邻节段的再手术率。
患者与方法-2007 年至 2012 年间,6532 例患者因 L4-5 椎管狭窄症合并或不合并 DS 接受手术治疗,随访至 2017 年,以确定指数和相邻节段的再手术情况。比较了减压融合与单纯减压以及合并或不合并 DS 的患者之间的再手术率。收集了患者术前、术后 1 年和 2 年的报告结果数据,用于评估指数手术和再手术之间结果的差异。
结果-对于合并 DS 的腰椎管狭窄症,减压融合的指数水平再手术率为 3.0%,单纯减压的再手术率为 6.0%。在相邻水平,相应的数字分别为 9.7%和 4.2%。对于不合并 DS 的腰椎管狭窄症,减压融合的指数水平再手术率为 3.7%,单纯减压的再手术率为 6.2%。在相邻水平,相应的数字分别为 8.1%和 3.8%。对于相邻水平的再手术,扩展融合与单纯减压之间的患者报告结果无差异。
结论-与单纯减压相比,单节段腰椎融合术与相邻节段再手术率增加相关。当包括指数水平的再手术时,融合与单纯减压的再手术率没有差异。