Department of Orthopaedic Surgery, Kanagawa Rehabilitation Hospital, 516 Nanasawa, Kanagawa, 516, 243-0121, Atsugi, Japan.
Department of Orthopaedic Surgery, The Jikei University School of Medicine, 3-19-18 Nishishinbashi, Minato-ku, 105-8471, Tokyo, Japan.
BMC Musculoskelet Disord. 2021 Feb 1;22(1):129. doi: 10.1186/s12891-021-04008-y.
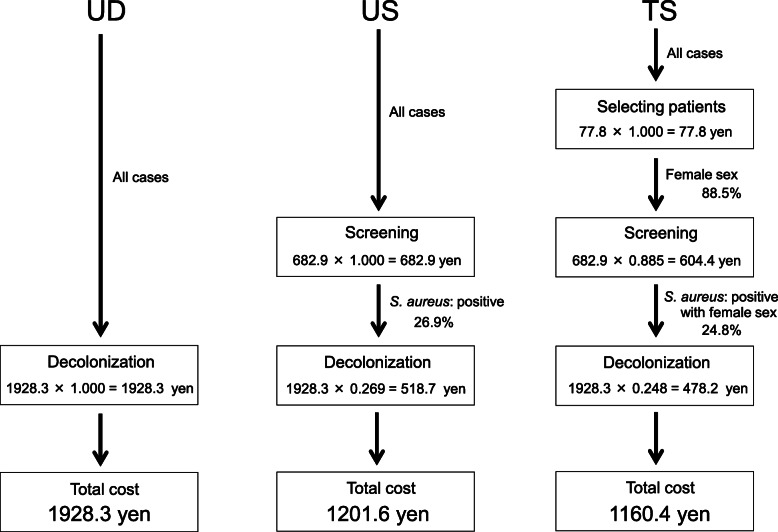
To reduce periprosthetic joint infection after total hip arthroplasty (THA), several nasal screening and decolonization strategies for methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-sensitive Staphylococcus aureus (MSSA) have been performed. These include universal decolonization (UD; i.e., no screening and decolonization for all patients), universal screening and target decolonization (US; i.e., screening for all patients and decolonization for bacterial positive patients), and target screening and decolonization (TS; i.e., screening and decolonization for high-risk populations only). Although TS is the most cost-effective strategy, useful risk factors must be identified. The purpose of this study was to evaluate the presence of predictive factors that enable the TS strategy to be successfully implemented and to compare the costs of each strategy.
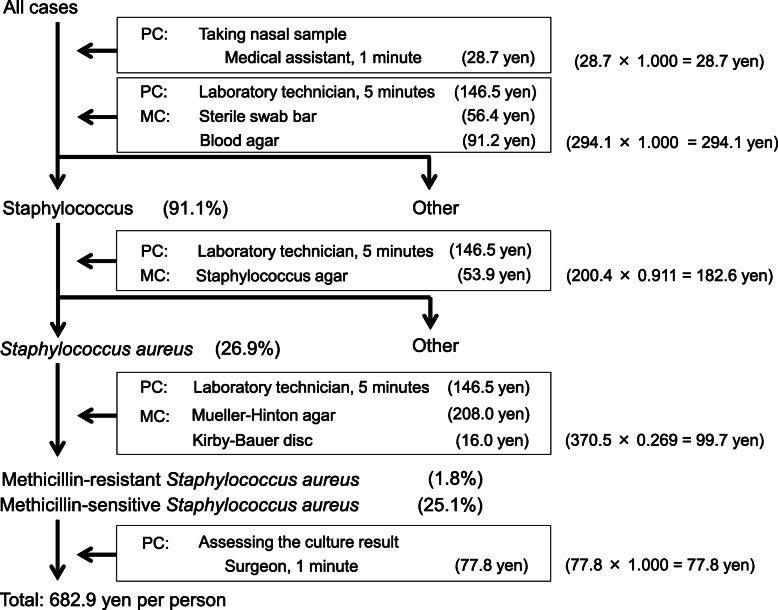
A total of 1654 patients scheduled for primary or revision THA (1464 female, 190 male; mean age 64 years) were screened prior to surgery for bacterial colonization of the nasal mucosa. Risk factors for positive MRSA and S. aureus (including both MRSA and MSSA) tests were analyzed according to the following parameters: sex, age ≥ 80 years, body mass index ≥ 30 kg/m, antibiotic use within 3 years, corticosteroid use, serum albumin < 3.5 g/dL, glomerular filtration rate < 50 mL/min, presence of brain, thyroid, cardiac, or pulmonary disease, diabetes, asthma, smoking status, and whether revision surgery was performed. The average cost of each strategy was calculated.
In total, 29 patients (1.8 %) tested positive for MRSA and 445 (26.9 %) tested positive for S. aureus. No parameters were identified as independent risk factors for MRSA and only female sex was identified as a risk factor for S. aureus (p = 0.003; odds ratio: 1.790; 95 % confidence interval: 1.210-2.640). The average cost of each strategy was 1928.3 yen for UD, 717.6 yen for US, and 717.6 yen for TS (for eradicating MRSA), and 1928.3 yen for UD, 1201.6 yen for US, and 1160.4 yen for TS (for eradicating S. aureus).
No useful predictive parameters for implementing the TS strategy were identified. Based on cost implications, US is the most cost-effective strategy for THA patients.
为了降低全髋关节置换术后(THA)的假体周围关节感染,已经针对耐甲氧西林金黄色葡萄球菌(MRSA)和甲氧西林敏感金黄色葡萄球菌(MSSA)实施了几种鼻腔筛查和去定植策略。这些策略包括普遍去定植(UD;即不对所有患者进行筛查和去定植)、普遍筛查和靶向去定植(US;即对所有患者进行筛查,对细菌阳性患者进行去定植)和靶向筛查和去定植(TS;即仅对高危人群进行筛查和去定植)。尽管 TS 是最具成本效益的策略,但必须确定有用的危险因素。本研究的目的是评估是否存在使 TS 策略能够成功实施的预测因素,并比较每种策略的成本。
共有 1654 名接受初次或翻修 THA 的患者(1464 名女性,190 名男性;平均年龄 64 岁)在手术前筛查鼻腔黏膜细菌定植情况。根据以下参数分析 MRSA 和金黄色葡萄球菌(包括 MRSA 和 MSSA)检测阳性的危险因素:性别、年龄≥80 岁、体重指数≥30kg/m、3 年内使用抗生素、使用皮质类固醇、血清白蛋白<3.5g/dL、肾小球滤过率<50ml/min、存在脑、甲状腺、心脏或肺部疾病、糖尿病、哮喘、吸烟状况以及是否进行翻修手术。计算每种策略的平均成本。
共有 29 名患者(1.8%)MRSA 检测阳性,445 名患者(26.9%)金黄色葡萄球菌检测阳性。没有发现任何参数是 MRSA 的独立危险因素,只有女性是金黄色葡萄球菌的危险因素(p=0.003;比值比:1.790;95%置信区间:1.210-2.640)。每种策略的平均成本分别为 UD 1928.3 日元、US 717.6 日元和 TS(根除 MRSA)717.6 日元,UD 1928.3 日元、US 1201.6 日元和 TS(根除金黄色葡萄球菌)1160.4 日元。
没有发现可用于实施 TS 策略的有用预测参数。基于成本考虑,US 是 THA 患者最具成本效益的策略。