Department of Radiation Oncology, Heidelberg University Hospital, Im Neuenheimer Feld 400, 69120, Heidelberg, Germany.
Department of Radiation Oncology, Heidelberg Institute of Radiation Oncology (HIRO), Heidelberg University Hospital, Heidelberg, Germany.
Radiat Oncol. 2021 Feb 1;16(1):23. doi: 10.1186/s13014-021-01749-x.
Radiation therapy and chemoradiation therapy play a major role in the definitive management of esophageal cancer. Survival in esophageal cancer patients is still relatively poor, mostly due to high rates of local recurrence and distant metastases. It is hypothesized that dose escalation in radiotherapy could improve outcomes. Therefore, this retrospective analysis aimed to investigate the outcomes and toxicity in patients treated with local dose escalation by means of using simultaneous integrated boost concepts.
Between 2012 and 2018, 101 patients with esophageal carcinoma were analyzed in this monocentric, retrospective study. All patients received definitive chemoradiation or radiation therapy alone as intensity modulated radiotherapy. The prescribed dose was 50.4 Gy in 28 fractions to the primary tumor and the elective lymph nodes as well as a simultaneous integrated boost (SIB) with 58.8 Gy to macroscopic tumor and lymph node metastases. Endpoints were overall survival (OS), progression free survival (PFS), local control rate (LCR) and toxicity.
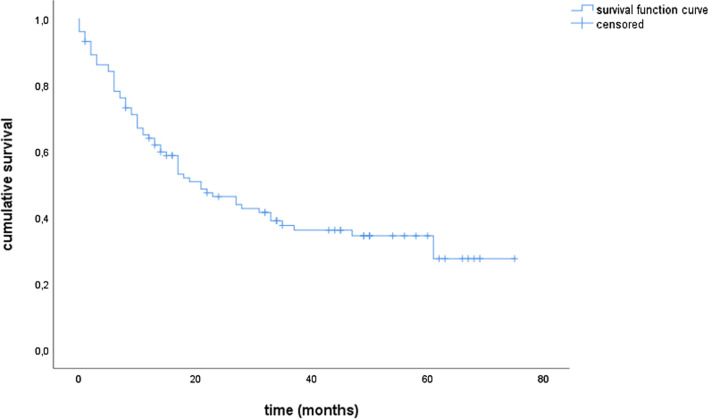
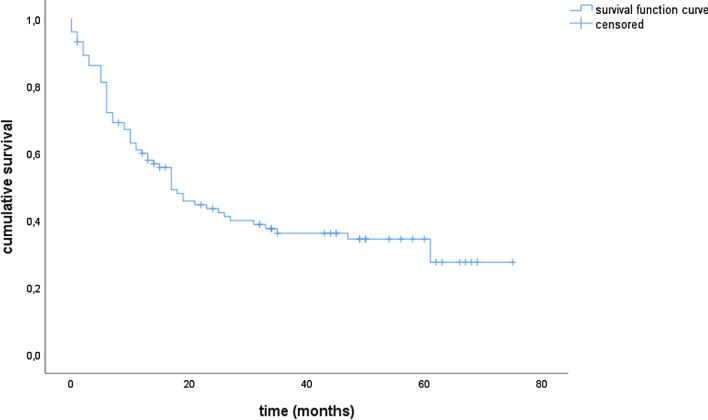
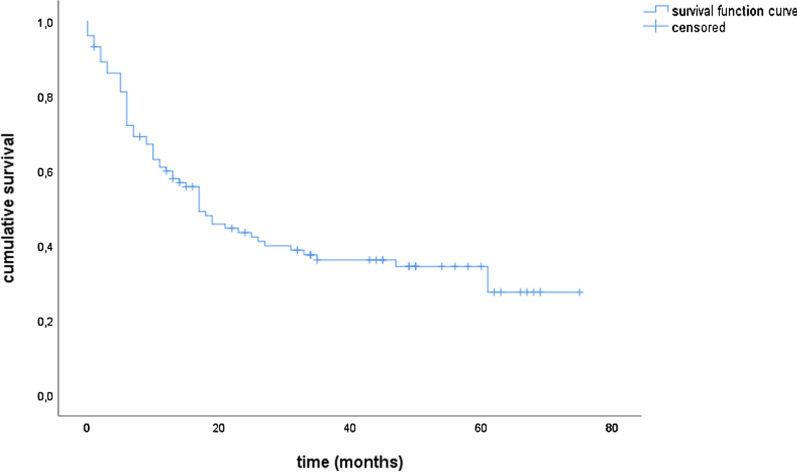
60 patients (59.4%) received chemoradiation, 41 patients (40.6%) radiotherapy alone. The median follow up was 17 months (range 0-75 months). OS, PFS and LCR were at 63.9%, 53.9% and 59.9% after 1 year and 37.6%, 34.5% and 36.1%, respectively after 3 years. 16 patients (15.8%) in total developed a locoregional recurrence within the field of radiation. In 48 patients (47.5%) at least one grade III° (CTCAE) toxicity was documented during radiotherapy, mostly dysphagia (36 pat., 75%). One patient suffered from a grade IV° pneumonia.
This retrospective analysis demonstrates that a SIB concept in definitive (chemo)radiation therapy is safe and feasible, showing acceptable outcomes in this patient cohort. Considering that this cohort mainly consists of elderly patients not eligible for chemotherapy in many cases, we emphasize the aspect of SIB radiation therapy as potential partial compensation for omitted simultaneous chemotherapy. Prospective studies are needed for validation.
放射治疗和放化疗在食管癌的确定性治疗中起着重要作用。食管癌患者的生存率仍然相对较低,主要是由于局部复发和远处转移的发生率较高。有人假设放射治疗的剂量升级可以改善结果。因此,这项回顾性分析旨在通过使用同步整合升压概念来研究接受局部剂量升级治疗的患者的结果和毒性。
在这项单中心回顾性研究中,分析了 2012 年至 2018 年间的 101 例食管癌患者。所有患者均接受根治性放化疗或单纯调强放疗。规定的剂量为原发肿瘤和选择性淋巴结 50.4Gy/28 次,同时对宏观肿瘤和淋巴结转移进行同步整合升压(SIB),剂量为 58.8Gy。终点是总生存期(OS)、无进展生存期(PFS)、局部控制率(LCR)和毒性。
60 例(59.4%)患者接受放化疗,41 例(40.6%)患者单纯放疗。中位随访时间为 17 个月(0-75 个月)。1 年时 OS、PFS 和 LCR 分别为 63.9%、53.9%和 59.9%,3 年后分别为 37.6%、34.5%和 36.1%。共有 16 例(15.8%)患者在放射治疗野内发生局部区域复发。48 例(47.5%)患者在放疗过程中至少发生了 1 级(CTCAE)毒性,主要为吞咽困难(36 例,75%)。1 例患者发生 4 级肺炎。
这项回顾性分析表明,在确定性(放化疗)治疗中采用 SIB 概念是安全可行的,在该患者队列中显示出可接受的结果。考虑到该队列主要由许多情况下不适合化疗的老年患者组成,我们强调 SIB 放疗作为同时省略化疗的潜在部分补偿的方面。需要前瞻性研究来验证。