Cardiovascular Center, Taichung Veterans General Hospital.
Division of Cardiology, Asia University Hospital.
Medicine (Baltimore). 2021 Jan 22;100(3):e23830. doi: 10.1097/MD.0000000000023830.
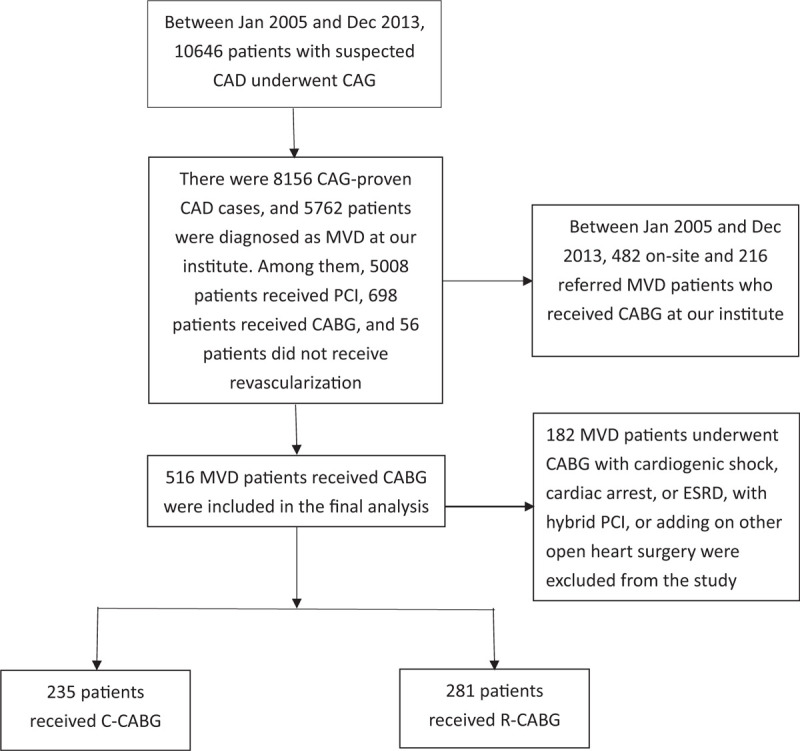
The treatment of patients with multivessel coronary artery disease (MVD) by coronary stenting (PCI) and the "gold standard" conventional coronary-artery bypass grafting (C-CABG) has been well explored in the literature. However, the clinical outcomes of robot-assisted CABG (R-CABG) vs C-CABG in MVD patients in real-world practice were unknown. We aimed to study the clinical outcomes of MVD patients who underwent R-CABG (robotic MIDCAB) and C-CABG at our institution between January 2005 and December 2013.A total of 516 MVD patients received CABG were recruited into this study. Among them, 281 patients received R-CABG and 235 patients underwent C-CABG. Patients in the R-CABG group were younger, and had fewer vessels with coronary artery disease (CAD), lower prevalence of chronic renal disease (CKD), higher left ventricular ejection fraction (LVEF), as well as lower Euro scores. The in-hospital and long-term mortalities were lower in the R-CABG group, but the incidences of target lesion revascularization (TLR), target vessel revascularization (TVR), myocardial infarction (MI), and stroke were not significantly different between the two groups. The long-term mortality was related to age, lower LVEF, and CKD, but not residual SYNTAX score, or completeness of revascularization. The revascularization modality (R-CABG vs C-CABG) was a borderline significantly independent predictor of long-term mortality (OR 1.76 [0.99-3.14], P = .055).Our study concluded that R-CABG, in comparison with C-CABG, for MVD carried out in younger patients involved fewer clinical complexities was associated with lower in-hospital and long-term mortalities in real-world practice. However, the long-term rates of TLR, TVR, MI, and stroke were similar. The long-term mortality was correlated with age, lower LVEF, and CKD, where R-CABG remained a borderline significant predictor after correcting for confounding factors. R-CABG could be an effective alternative to C-CABG for MVD patients with fewer clinical complexities in real-world practice.
在文献中已经充分探讨了经皮冠状动脉介入治疗(PCI)和冠状动脉旁路移植术(CABG)治疗多支血管病变(MVD)患者的情况。然而,在真实世界实践中,机器人辅助 CABG(R-CABG)与 CABG 治疗 MVD 患者的临床结果尚不清楚。我们旨在研究 2005 年 1 月至 2013 年 12 月期间在我院接受 R-CABG(机器人 MIDCAB)和 C-CABG 的 MVD 患者的临床结果。
这项研究共纳入了 516 例接受 CABG 的 MVD 患者。其中,281 例患者接受 R-CABG,235 例患者接受 C-CABG。R-CABG 组患者更年轻,冠状动脉疾病(CAD)血管较少,慢性肾脏病(CKD)患病率较低,左心室射血分数(LVEF)较高,Euro 评分较低。R-CABG 组患者的住院和长期死亡率较低,但两组患者的靶病变血运重建(TLR)、靶血管血运重建(TVR)、心肌梗死(MI)和中风发生率无显著差异。长期死亡率与年龄、较低的 LVEF 和 CKD 有关,但与残余 SYNTAX 评分或血运重建的完整性无关。血运重建方式(R-CABG 与 C-CABG)是长期死亡率的一个边缘显著独立预测因素(OR 1.76 [0.99-3.14],P=0.055)。
我们的研究表明,与 C-CABG 相比,在真实世界实践中,对于年轻患者进行的 MVD,R-CABG 涉及的临床复杂性较少,与住院和长期死亡率较低相关。然而,TLR、TVR、MI 和中风的长期发生率相似。长期死亡率与年龄、较低的 LVEF 和 CKD 相关,在纠正混杂因素后,R-CABG 仍然是一个边缘显著的预测因素。在真实世界实践中,对于临床复杂性较少的 MVD 患者,R-CABG 可以作为 C-CABG 的有效替代方法。