Soldati Salvatore, Di Martino Mirko, Castagno Davide, Davoli Marina, Fusco Danilo
Department of Epidemiology, Lazio Regional Health Service, Rome, Italy.
Department of Epidemiology, Lazio Regional Health Service, Rome, Italy
BMJ Open. 2021 Feb 5;11(2):e042878. doi: 10.1136/bmjopen-2020-042878.
This study aimed to measure adherence to chronic polytherapy following an acute myocardial infarction (AMI) and to find out associations between adherence and the setting of AMI onset (in vs out of hospital) as well as other determinants.
Retrospective follow-up study.
Population living in the Lazio Region, Italy.
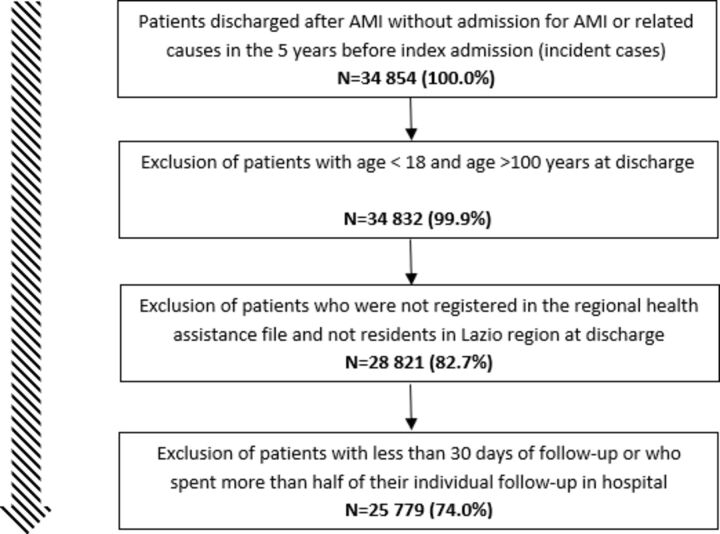
This study included 25 779 hospitalised patients with a first diagnosis of AMI in 2012-2016, after the exclusion of those with hospital admission for AMI or related causes in the previous 5 years.
Patients were classified as in-hospital AMI (IH-AMI) or out of hospital AMI (OH-AMI) according to present-on-admission codes. Adherence was measured based on prescription claims during a 6-month follow-up after hospital discharge, using medication possession ratio (MPR). Adherence to chronic polytherapy was defined as MPR ≥75% to at least 3 of the following medications: antithrombotics, betablockers, ACE inhibitors/angiotensin receptor blockers and statins.
Among the entire cohort, 1 044 (4%) patients suffered IH-AMI. Overall, 15 440 (60%) patients were deemed adherent to chronic polytherapy. Female gender, older age, mental disorders, renal disease, asthma and ongoing concomitant treatments were factors associated with poor adherence. By contrast, patients with more severe AMI and those already taking evidence-based (E-B) drugs were more likely to be adherent. A strong association between the setting of AMI onset and adherence was observed: IH-AMI patients were 46% less likely to be adherent to E-B medications during their 6-month follow-up as compared with OH-AMI patients (OR 0.54; 95% CI 0.47 to 0.62; p<0.001).
Pharmacotherapy is not consistent with clinical guidelines, especially for IH-AMI patients. Our findings provide evidence on a previously unidentified groups of patients at risk for poor adherence, who might benefit from greater medical attention and dedicated healthcare interventions.
本研究旨在衡量急性心肌梗死(AMI)后慢性联合治疗的依从性,并找出依从性与AMI发病地点(院内与院外)以及其他决定因素之间的关联。
回顾性随访研究。
居住在意大利拉齐奥地区的人群。
本研究纳入了2012年至2016年首次诊断为AMI的25779例住院患者,排除了过去5年内因AMI或相关原因入院的患者。
根据入院时的编码将患者分为院内AMI(IH-AMI)或院外AMI(OH-AMI)。出院后6个月的随访期间,根据处方记录,使用药物持有率(MPR)来衡量依从性。慢性联合治疗的依从性定义为MPR≥75%,且至少对以下药物中的3种:抗血栓药、β受体阻滞剂、ACE抑制剂/血管紧张素受体阻滞剂和他汀类药物。
在整个队列中,1044例(4%)患者发生IH-AMI。总体而言,15440例(60%)患者被认为对慢性联合治疗依从。女性、年龄较大、精神障碍、肾病、哮喘和正在进行的联合治疗是与依从性差相关的因素。相比之下,AMI更严重的患者和已经在服用循证(E-B)药物的患者更有可能依从。观察到AMI发病地点与依从性之间存在强烈关联:与OH-AMI患者相比,IH-AMI患者在6个月随访期间对E-B药物的依从性降低46%(OR 0.54;95%CI 0.47至0.62;p<0.001)。
药物治疗与临床指南不一致,尤其是对于IH-AMI患者。我们的研究结果为先前未识别的依从性差风险患者群体提供了证据,这些患者可能受益于更多的医疗关注和专门的医疗保健干预措施。