Angelo Bianchi Bonomi Hemophilia and Thrombosis Center and Fondazione Luigi Villa, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy.
Department of Pathophysiology and Transplantation, Università degli Studi di Milano, Milan, Italy.
Front Immunol. 2021 Jan 22;11:591878. doi: 10.3389/fimmu.2020.591878. eCollection 2020.
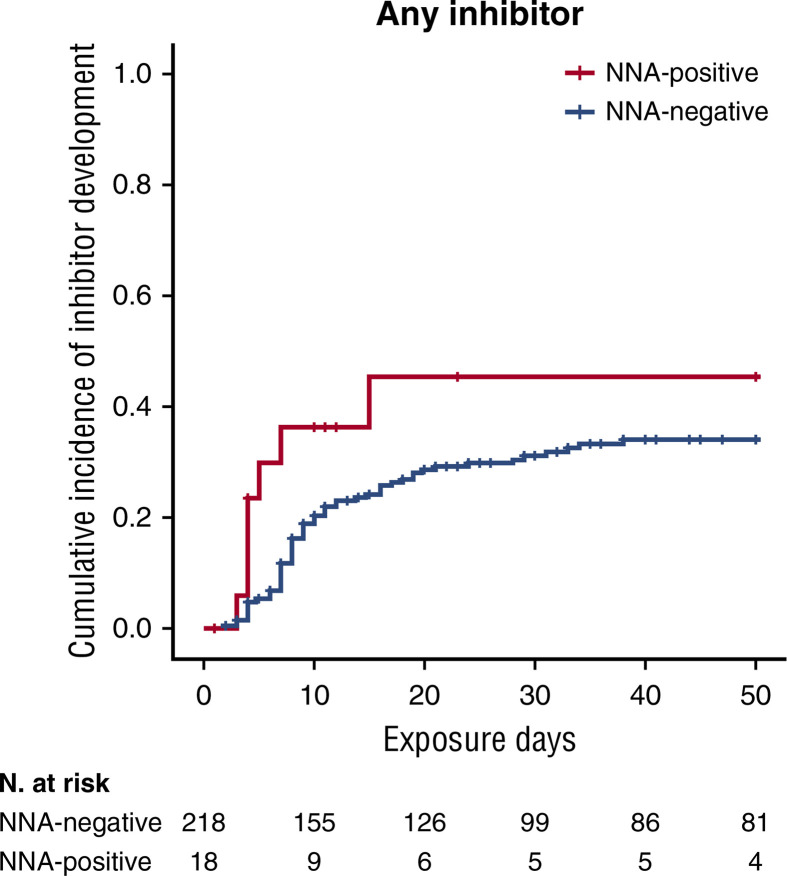
The most severe side effect of hemophilia treatment is the inhibitor development occurring in 30% of patients, during the earliest stages of treatment with factor (F)VIII concentrates. These catastrophic immune responses rapidly inactivate the infused FVIII, rendering the treatment ineffective. This complication is associated with a substantial morbidity and mortality. The risk factors involved in the onset of the inhibitors are both genetic and environmental. The source of FVIII products, i.e. plasma-derived or recombinant FVIII products, is considered one of the most relevant factors for inhibitor development. Numerous studies in the literature report conflicting data on the different immunogenicity of the products. The SIPPET randomized trial showed an increased in the inhibitor rate in patients using recombinant FVIII products than those receiving plasma-derived products in the first exposure days. The SIPPET randomized trial showed an increase in the inhibitor rate in patients using recombinant FVIII products compared to those treated with plasma-derived products in the first days of exposure. The potential increase in the immunogenicity of recombinant products can be attributed to several factors such as: the different post-translational modification in different cell lines, the presence of protein aggregates, and the role played by the chaperon protein of FVIII, the von Willebrand factor, which modulates the uptake of FVIII by antigen presenting cells (APCs). Furthermore, the presence of non-neutralizing antibodies against FVIII has shown to be in increased inhibitor development as demonstrated in a sub-analysis of the SIPPET study. In addition, the presence of the specific subclasses of the immunoglobulins may also be an important biomarker to indicate whether the inhibitor will evolve into a persistent neutralizing antibody or a transient one that would disappear without any specific treatment. Recently, the availability of novel non-replacement therapies as well as emicizumab, administered by weekly subcutaneous infusion, have significantly changed the quality of life of patients with inhibitors showing a considerable reduction of the annual bleeding rate and in most patients the absence of bleeding. Although, these novel drugs improve patients' quality of life, they do not abolish the need to infuse FVIII during acute bleeding or surgery. Therefore, the issue of immunogenicity against FVIII still remains an important side effect of hemophilia treatment.
血友病治疗最严重的副作用是抑制剂的发展,在接受因子(F)VIII 浓缩物治疗的最初阶段,30%的患者会出现这种灾难性的免疫反应。这些快速的免疫反应迅速使输注的 FVIII 失活,使治疗无效。这种并发症与大量的发病率和死亡率有关。抑制剂发生的危险因素既有遗传的也有环境的。FVIII 产品的来源,即血浆衍生或重组 FVIII 产品,被认为是抑制剂发展的最相关因素之一。文献中有许多研究报告了产品免疫原性的相互矛盾的数据。SIPPET 随机试验显示,在首次接触的几天内,使用重组 FVIII 产品的患者的抑制剂发生率高于使用血浆衍生产品的患者。SIPPET 随机试验显示,在首次接触的几天内,使用重组 FVIII 产品的患者的抑制剂发生率高于使用血浆衍生产品的患者。重组产品免疫原性的潜在增加可归因于以下几个因素:不同细胞系中不同的翻译后修饰、蛋白质聚集的存在以及 FVIII 伴侣蛋白 von Willebrand 因子(调节 APC 摄取 FVIII 的作用)。此外,非中和性抗 FVIII 抗体的存在已被证明与抑制剂的发展有关,正如 SIPPET 研究的亚分析所示。此外,免疫球蛋白的特定亚类的存在也可能是一个重要的生物标志物,表明抑制剂是否会发展为持续的中和抗体或会在没有任何特定治疗的情况下消失的短暂的非中和抗体。最近,新型非替代疗法以及emicizumab(每周皮下输注)的出现,极大地改变了抑制剂患者的生活质量,显著降低了年出血率,在大多数患者中没有出血。尽管这些新型药物改善了患者的生活质量,但它们并没有消除在急性出血或手术期间输注 FVIII 的需要。因此,针对 FVIII 的免疫原性仍然是血友病治疗的一个重要副作用。