Matsushima Masaaki, Yabe Ichiro, Sakushima Ken, Kanatani Yasuhiro, Nishimoto Naoki, Matsuoka Takeshi, Sawada Jun, Uesugi Haruo, Sako Kazuya, Takei Asako, Tamakoshi Akiko, Shimohama Shun, Sato Norihiro, Kikuchi Seiji, Sasaki Hidenao
Department of Neurology, Hokkaido University Graduate School of Medicine, Sapporo, Hokkaido, Japan
Department of Neurology, Hokkaido University Graduate School of Medicine, Sapporo, Hokkaido, Japan.
BMJ Open. 2021 Feb 8;11(2):e045100. doi: 10.1136/bmjopen-2020-045100.
Multiple system atrophy (MSA) is a refractory neurodegenerative disease, but novel treatments are anticipated. An accurate natural history of MSA is important for clinical trials, but is insufficient. This regional registry was launched to complement clinical information on MSA.
Patient recruitment started in November 2014 and is ongoing at the time of submission. The number of participating facilities was 66. Postal surveys were sent to medical facilities and patients with MSA in Hokkaido, Japan.
After obtaining written consent from 196 participants, 184 overview surveys and 115 detailed surveys were conducted.
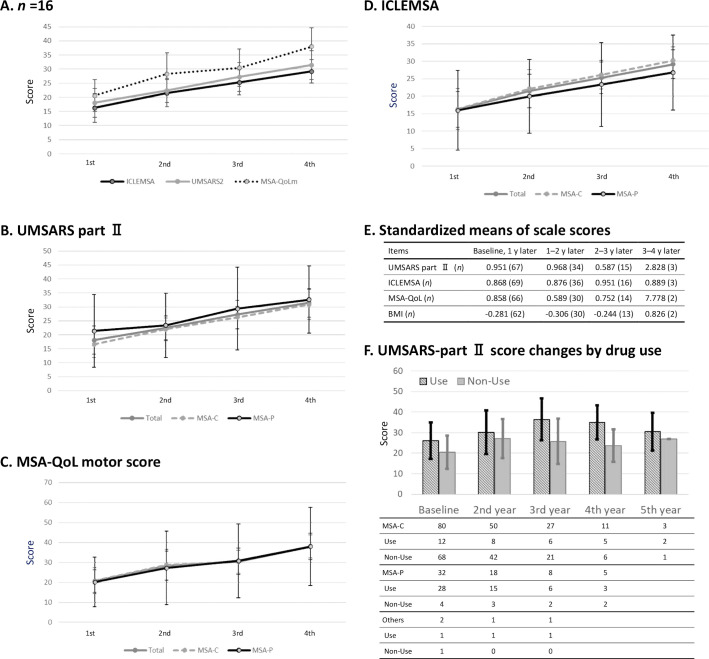
An overview survey evaluated conformity to diagnostic criteria and a detailed survey implemented an annual assessment based on the Unified Multiple System Atrophy Rating Scale (UMSARS).
At the time of registration, 58.2% of patients were diagnosed with cerebellar symptoms predominant type MSA (MSA-C) and 29.9% were diagnosed with parkinsonism predominant type MSA (MSA-P). UMSARS Part Ⅳ score of 4 or 5 accounted for 53.8% of participants. The higher the UMSARS Part Ⅳ score, the higher the proportion of MSA-P. At baseline, levodopa was used by 69 patients (37.5%) and the average levodopa dose was 406.7 mg/day. The frequency of levodopa use increased over time. Eleven cases changed from MSA-C to MSA-P during the study, but the opposite was not observed. Information about survival and causes of death was collected on 54 cases. Half of deaths were respiratory-related. Sudden death was recorded even in the group with UMSARS Part Ⅳ score of 1.
This study is the first large-scale prospective MSA cohort study in Asia. MSA-C was dominant, but the use of antiparkinsonian drugs increased over the study period. Changes from MSA-C to MSA-P occurred, but not vice versa.
多系统萎缩(MSA)是一种难治性神经退行性疾病,但有望出现新的治疗方法。准确的MSA自然史对临床试验很重要,但目前尚不充分。启动该地区登记系统以补充MSA的临床信息。
患者招募于2014年11月开始,在提交本文时仍在进行中。参与机构有66家。向日本北海道的医疗机构和MSA患者发送了邮政调查问卷。
在获得196名参与者的书面同意后,进行了184份概述调查和115份详细调查。
概述调查评估对诊断标准的符合情况,详细调查基于统一多系统萎缩评定量表(UMSARS)进行年度评估。
登记时,58.2%的患者被诊断为以小脑症状为主型MSA(MSA-C),29.9%被诊断为以帕金森综合征为主型MSA(MSA-P)。UMSARS第四部分得分为4或5的参与者占53.8%。UMSARS第四部分得分越高,MSA-P的比例越高。基线时,69名患者(37.5%)使用左旋多巴,平均左旋多巴剂量为406.7毫克/天。左旋多巴的使用频率随时间增加。研究期间有11例从MSA-C转变为MSA-P,但未观察到相反情况。收集了54例患者的生存和死亡原因信息。一半的死亡与呼吸相关。即使在UMSARS第四部分得分为1的组中也记录到了猝死。
本研究是亚洲首个大规模前瞻性MSA队列研究。MSA-C占主导,但在研究期间抗帕金森病药物的使用增加。发生了从MSA-C到MSA-P的转变,但反之则未发生。