Mutinelli-Szymanski Prisca, Hude Iulia, Merle Emilie, Lombardi Yannis, Seris Pascal, Abtahi Medhi, Azeroual Latifa, Bourgain Cecile, Ensergueix Gael, Katerinis Ioannis, Kolko Anne, Kolta Amir, Maheas Catherine, Mehrbanian Saeed, Morel Pauline, Ossman Rim, de Préneuf Hélène, Roux Arthur, Saltiel Claudine, Vendé Florence, Verhoeven Anne-Sophie, Viron Béatrice, Laplanche Sophie, Le Monnier Alban, Ridel Christophe, Ureña-Torres Pablo, Touzot Maxime
AURA Saint-Ouen, Dialyse, Saint-Ouen, France.
AURA Paris Plaisance, Dialyse et aphérèse thérapeutique, Paris, France.
Clin Kidney J. 2020 Nov 21;14(1):124-131. doi: 10.1093/ckj/sfaa194. eCollection 2021 Jan.
Information regarding coronavirus disease 2019 (COVID-19) in haemodialysis (HD) patients is limited and early studies suggest a poor outcome. We aimed to identify clinical and biological markers associated with severe forms of COVID-19 in HD patients.
We conducted a prospective, observational and multicentric study. Sixty-two consecutive adult HD patients with confirmed COVID-19 from four dialysis facilities in Paris, France, from 19 March to 19 May 2020 were included.Blood tests were performed before diagnosis and at Days 7 and 14 after diagnosis. Severe forms of COVID-19 were defined as requiring oxygen therapy, admission in an intensive care unit or death. Cox regression models were used to compute adjusted hazard ratios (aHRs). Kaplan-Meier curves and log-rank tests were used for survival analysis.
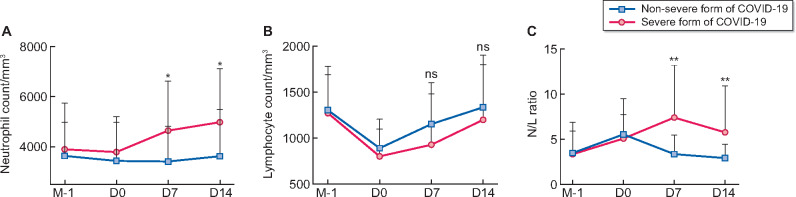
Twenty-eight patients (45%) displayed severe forms of COVID-19. Compared with non-severe forms, these patients had more fever (93% versus 56%, P < 0.01), cough (71% versus 38%, P = 0.02) and dyspnoea (43% versus 6%, P < 0.01) at diagnosis. At Day 7 post-diagnosis, neutrophil counts, neutrophil:lymphocyte (N:L) ratio, C-reactive protein, ferritin, fibrinogen and lactate dehydrogenase levels were significantly higher in severe COVID-19 patients. Multivariate analysis revealed an N:L ratio >3.7 was the major marker associated with severe forms, with an aHR of 4.28 (95% confidence interval 1.52-12.0; P = 0.006). After a median follow-up time of 48 days (range 27-61), six patients with severe forms died (10%).
HD patients are at increased risk of severe forms of COVID-19. An elevated N:L ratio at Day 7 was highly associated with the severe forms. Assessing the N:L ratio could inform clinicians for early treatment decisions.
关于血液透析(HD)患者感染2019冠状病毒病(COVID-19)的信息有限,早期研究表明其预后较差。我们旨在确定与HD患者中重症COVID-19相关的临床和生物学标志物。
我们开展了一项前瞻性、观察性多中心研究。纳入了2020年3月19日至5月19日期间来自法国巴黎四个透析机构的62例连续确诊COVID-19的成年HD患者。在诊断前以及诊断后第7天和第14天进行血液检测。重症COVID-19定义为需要氧疗、入住重症监护病房或死亡。采用Cox回归模型计算调整后的风险比(aHRs)。采用Kaplan-Meier曲线和对数秩检验进行生存分析。
28例患者(45%)表现为重症COVID-19。与非重症患者相比,这些患者在诊断时有更多发热(93%对56%,P<0.01)、咳嗽(71%对38%,P=0.02)和呼吸困难(43%对6%,P<0.01)。在诊断后第7天,重症COVID-19患者的中性粒细胞计数、中性粒细胞与淋巴细胞(N:L)比值、C反应蛋白、铁蛋白、纤维蛋白原和乳酸脱氢酶水平显著更高。多变量分析显示,N:L比值>3.7是与重症形式相关的主要标志物,aHR为4.28(95%置信区间1.52-12.0;P=0.006)。在中位随访时间48天(范围27-61天)后,6例重症患者死亡(10%)。
HD患者发生重症COVID-19的风险增加。第7天N:L比值升高与重症形式高度相关。评估N:L比值可为临床医生的早期治疗决策提供依据。