Mayne Kaitlin J, Lees Jennifer S, Rutherford Elaine, Thomson Peter C, Traynor Jamie P, Dey Vishal, Lang Ninian N, Mark Patrick B
School of Cardiovascular & Metabolic Health, University of Glasgow, Glasgow, UK.
Glasgow Renal and Transplant Unit, Queen Elizabeth University Hospital, Glasgow, UK.
Clin Kidney J. 2022 Nov 18;16(3):512-520. doi: 10.1093/ckj/sfac248. eCollection 2023 Mar.
Lymphocyte ratios reflect inflammation and have been associated with adverse outcomes in a range of diseases. We sought to determine any association between neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) and mortality in a haemodialysis cohort, including a coronavirus disease 2019 (COVID-19) infection subpopulation.
A retrospective analysis was performed of adults commencing hospital haemodialysis in the West of Scotland during 2010-21. NLR and PLR were calculated from routine samples around haemodialysis initiation. Kaplan-Meier and Cox proportional hazards analyses were used to assess mortality associations.
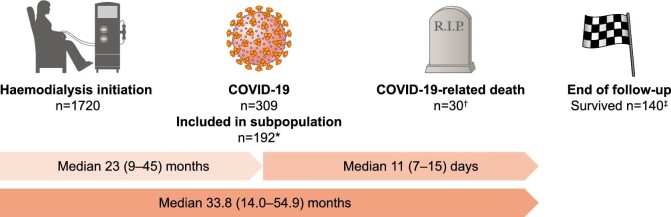
In 1720 haemodialysis patients over a median of 21.9 (interquartile range 9.1-42.9) months, there were 840 all-cause deaths. NLR but not PLR was associated with all-cause mortality after multivariable adjustment [adjusted hazard ratio (aHR) for in participants with baseline NLR in quartile 4 (NLR ≥8.23) versus quartile 1 (NLR <3.12) 1.63, 95% confidence interval (CI) 1.32-2.00]. The association was stronger for cardiovascular death (NLR quartile 4 versus 1 aHR 3.06, 95% CI 1.53-6.09) than for non-cardiovascular death (NLR quartile 4 versus 1 aHR 1.85, 95% CI 1.34-2.56). In the COVID-19 subpopulation, both NLR and PLR at haemodialysis initiation were associated with risk of COVID-19-related death after adjustment for age and sex (NLR: aHR 4.69, 95% CI 1.48-14.92 and PLR: aHR 3.40, 95% CI 1.02-11.36; for highest vs lowest quartiles).
NLR is strongly associated with mortality in haemodialysis patients while the association between PLR and adverse outcomes is weaker. NLR is an inexpensive, readily available biomarker with potential utility in risk stratification of haemodialysis patients.
淋巴细胞比例反映炎症反应,并且在一系列疾病中与不良预后相关。我们试图确定在一个血液透析队列中,包括2019冠状病毒病(COVID-19)感染亚组,中性粒细胞与淋巴细胞比值(NLR)和血小板与淋巴细胞比值(PLR)与死亡率之间是否存在关联。
对2010年至2021年期间在苏格兰西部开始进行医院血液透析的成年人进行回顾性分析。NLR和PLR通过血液透析开始时的常规样本计算得出。采用Kaplan-Meier法和Cox比例风险分析法评估死亡率的关联。
在1720例血液透析患者中,中位随访时间为21.9(四分位间距9.1 - 42.9)个月,全因死亡840例。多变量调整后,NLR而非PLR与全因死亡率相关[四分位4(NLR≥8.23)的参与者与四分位1(NLR<3.12)的参与者相比,调整后风险比(aHR)为1.63,95%置信区间(CI)为1.32 - 2.00]。心血管死亡的关联(NLR四分位4与1相比,aHR为3.06,95%CI为1.53 - 6.09)比非心血管死亡更强(NLR四分位4与1相比,aHR为小1.85,95%CI为1.34 - 2.56)。在COVID-19亚组中,血液透析开始时的NLR和PLR在调整年龄和性别后均与COVID-19相关死亡风险相关(NLR:aHR为4.69,95%CI为1.48 - 14.92;PLR:aHR为3.40,95%CI为1.02 - 11.36;最高四分位与最低四分位相比)。
NLR与血液透析患者的死亡率密切相关,而PLR与不良预后的关联较弱。NLR是一种廉价、易于获取的生物标志物,在血液透析患者的风险分层中具有潜在应用价值。