From the Department of Colorectal Surgery, Cleveland Clinic Foundation, Cleveland, Ohio, USA (Feinberg); the Department of Surgery, University of Toronto, Toronto, Ont. (Acuna); the Department of Surgery, North York General Hospital, Toronto, Ont. (Smith); the Department of Anesthesia, North York General Hospital, Toronto, Ont. (Kashin, Mocon, Yau, Srikandarajah) and the Department of Pharmacy, North York General Hospital, Toronto, Ont. (Chiu).
Can J Surg. 2021 Feb 9;64(1):E69-E75. doi: 10.1503/cjs.001319.
There has been an increase in opioid usage and opioid-related deaths. Opioids prescribed to surgical patients have similarly increased. The aim of this study was to assess opioid consumption in patients undergoing laparoscopic appendectomy (LA) and laparoscopic cholecystectomy (LC) and to determine whether a standardized prescription could affect opioid consumption without affecting patient satisfaction.
Patients undergoing LA or LC were recruited prospectively during 2 time periods (April to June 2017 and November 2017 to January 2018). In the first phase, surgeons continued their usual postoperative analgesia prescribing patterns. In the second phase, a standardized prescription was implemented. Patients were contacted by telephone and a questionnaire was completed for both phases of the study. The primary outcome was the quantity of opioids prescribed and consumed.
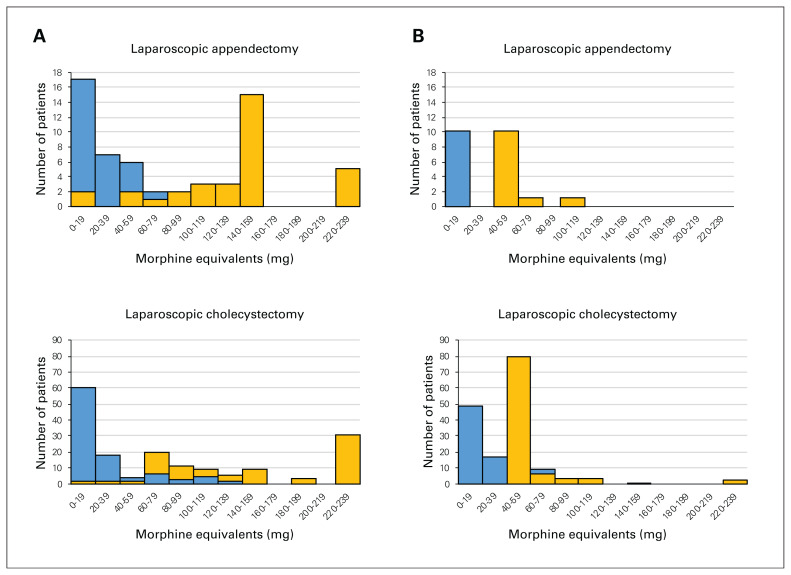
In the first phase, 166 patients who underwent LC or LA were recruited. The median number of prescribed opioid tablets was 20 and the median number consumed was 2. Ninety-five percent of patients reported satisfaction with their analgesia. Based on these results, a standardized prescription for multimodal analgesia was implemented for the second phase, consisting of 10 opioid tablets. In the second phase, 129 patients who underwent LA or LC were recruited. There was a significant decrease in the median number of opioid pills filled (10) and consumed (0), with no difference in reported satisfaction with analgesia.
Patients are prescribed an excess of opioids after LA or LC. Implementation of a standardized prescription based on a quality improvement intervention was effective at decreasing the number of opioids prescribed and consumed.
阿片类药物的使用和与阿片类药物相关的死亡人数有所增加。给外科患者开的阿片类药物也同样增加了。本研究的目的是评估行腹腔镜阑尾切除术(LA)和腹腔镜胆囊切除术(LC)患者的阿片类药物使用情况,并确定标准化处方是否可以在不影响患者满意度的情况下影响阿片类药物的使用。
在两个时间段(2017 年 4 月至 6 月和 2017 年 11 月至 2018 年 1 月)前瞻性地招募接受 LA 或 LC 的患者。在第一阶段,外科医生继续按照他们通常的术后镇痛处方模式进行治疗。在第二阶段,实施了标准化处方。在两个阶段的研究中,通过电话联系患者并完成了一份问卷。主要结果是开出处方和消耗的阿片类药物的数量。
在第一阶段,招募了 166 名接受 LC 或 LA 的患者。开出处方的阿片类药物片剂中位数为 20 片,消耗的中位数为 2 片。95%的患者报告对他们的镇痛效果满意。基于这些结果,为第二阶段实施了一种多模式镇痛的标准化处方,包括 10 片阿片类药物。在第二阶段,招募了 129 名接受 LA 或 LC 的患者。填充的阿片类药物片剂数量(10 片)和消耗的阿片类药物片剂数量(0 片)显著减少,而对镇痛效果的满意度没有差异。
LA 或 LC 后患者开出处方的阿片类药物过多。实施基于质量改进干预的标准化处方可有效减少处方和消耗的阿片类药物数量。