Oliphant Nicholas P, Manda Samuel, Daniels Karen, Odendaal Willem A, Besada Donela, Kinney Mary, White Johansson Emily, Doherty Tanya
The Global Fund to Fight AIDS, Tuberculosis, and Malaria, Geneva, Switzerland.
School of Public Health, University of the Western Cape, Belleville, South Africa.
Cochrane Database Syst Rev. 2021 Feb 10;2(2):CD012882. doi: 10.1002/14651858.CD012882.pub2.
The leading causes of mortality globally in children younger than five years of age (under-fives), and particularly in the regions of sub-Saharan Africa (SSA) and Southern Asia, in 2018 were infectious diseases, including pneumonia (15%), diarrhoea (8%), malaria (5%) and newborn sepsis (7%) (UNICEF 2019). Nutrition-related factors contributed to 45% of under-five deaths (UNICEF 2019). World Health Organization (WHO) and United Nations Children's Fund (UNICEF), in collaboration with other development partners, have developed an approach - now known as integrated community case management (iCCM) - to bring treatment services for children 'closer to home'. The iCCM approach provides integrated case management services for two or more illnesses - including diarrhoea, pneumonia, malaria, severe acute malnutrition or neonatal sepsis - among under-fives at community level (i.e. outside of healthcare facilities) by lay health workers where there is limited access to health facility-based case management services (WHO/UNICEF 2012).
To assess the effects of the integrated community case management (iCCM) strategy on coverage of appropriate treatment for childhood illness by an appropriate provider, quality of care, case load or severity of illness at health facilities, mortality, adverse events and coverage of careseeking for children younger than five years of age in low- and middle-income countries.
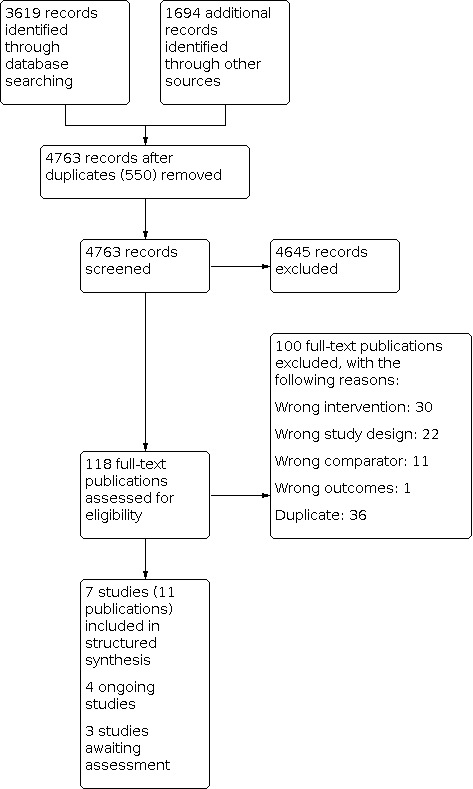
We searched CENTRAL, MEDLINE, Embase and CINAHL on 7 November 2019, Virtual Health Library on 8 November 2019, and Popline on 5 December 2018, three other databases on 22 March 2019 and two trial registers on 8 November 2019. We performed reference checking, and citation searching, and contacted study authors to identify additional studies.
Randomized controlled trials (RCTs), cluster-RCTs, controlled before-after studies (CBAs), interrupted time series (ITS) studies and repeated measures studies comparing generic WHO/UNICEF iCCM (or local adaptation thereof) for at least two iCCM diseases with usual facility services (facility treatment services) with or without single disease community case management (CCM). We included studies reporting on coverage of appropriate treatment for childhood illness by an appropriate provider, quality of care, case load or severity of illness at health facilities, mortality, adverse events and coverage of careseeking for under-fives in low- and middle-income countries.
At least two review authors independently screened abstracts, screened full texts and extracted data using a standardised data collection form adapted from the EPOC Good Practice Data Collection Form. We resolved any disagreements through discussion or, if required, we consulted a third review author not involved in the original screening. We contacted study authors for clarification or additional details when necessary. We reported risk ratios (RR) for dichotomous outcomes and hazard ratios (HR) for time to event outcomes, with 95% confidence intervals (CI), adjusted for clustering, where possible. We used estimates of effect from the primary analysis reported by the investigators, where possible. We analysed the effects of randomized trials and other study types separately. We used the GRADE approach to assess the certainty of evidence.
We included seven studies, of which three were cluster RCTs and four were CBAs. Six of the seven studies were in SSA and one study was in Southern Asia. The iCCM components and inputs were fairly consistent across the seven studies with notable variation for the training and deployment component (e.g. on payment of iCCM providers) and the system component (e.g. on improving information systems). When compared to usual facility services, we are uncertain of the effect of iCCM on coverage of appropriate treatment from an appropriate provider for any iCCM illness (RR 0.96, 95% CI 0.77 to 1.19; 2 CBA studies, 5898 children; very low-certainty evidence). iCCM may have little to no effect on neonatal mortality (HR 1.01, 95% 0.73 to 1.28; 2 trials, 65,209 children; low-certainty evidence). We are uncertain of the effect of iCCM on infant mortality (HR 1.02, 95% CI 0.83 to 1.26; 2 trials, 60,480 children; very low-certainty evidence) and under-five mortality (HR 1.18, 95% CI 1.01 to 1.37; 1 trial, 4729 children; very low-certainty evidence). iCCM probably increases coverage of careseeking to an appropriate provider for any iCCM illness by 68% (RR 1.68, 95% CI 1.24 to 2.27; 2 trials, 9853 children; moderate-certainty evidence). None of the studies reported quality of care, severity of illness or adverse events for this comparison. When compared to usual facility services plus CCM for malaria, we are uncertain of the effect of iCCM on coverage of appropriate treatment from an appropriate provider for any iCCM illness (very low-certainty evidence) and iCCM may have little or no effect on careseeking to an appropriate provider for any iCCM illness (RR 1.06, 95% CI 0.97 to 1.17; 1 trial, 811 children; low-certainty evidence). None of the studies reported quality of care, case load or severity of illness at health facilities, mortality or adverse events for this comparison.
AUTHORS' CONCLUSIONS: iCCM probably increases coverage of careseeking to an appropriate provider for any iCCM illness. However, the evidence presented here underscores the importance of moving beyond training and deployment to valuing iCCM providers, strengthening health systems and engaging community systems.
2018年,全球五岁以下儿童(尤其是撒哈拉以南非洲地区和南亚地区)的主要死因是传染病,包括肺炎(15%)、腹泻(8%)、疟疾(5%)和新生儿败血症(7%)(联合国儿童基金会,2019年)。与营养相关的因素导致了45%的五岁以下儿童死亡(联合国儿童基金会,2019年)。世界卫生组织(WHO)和联合国儿童基金会(UNICEF)与其他发展伙伴合作,制定了一种方法——现在称为综合社区病例管理(iCCM)——以使儿童治疗服务“更贴近家庭”。iCCM方法由非专业卫生工作者在社区层面(即医疗机构之外)为五岁以下儿童提供针对两种或更多疾病(包括腹泻、肺炎、疟疾、重度急性营养不良或新生儿败血症)的综合病例管理服务,前提是获得基于医疗机构的病例管理服务的机会有限(WHO/UNICEF,2012年)。
评估综合社区病例管理(iCCM)策略对中低收入国家五岁以下儿童获得适当提供者进行的儿童疾病适当治疗的覆盖率、医疗质量、医疗机构的病例负担或疾病严重程度、死亡率、不良事件以及寻求治疗的覆盖率的影响。
我们于2019年11月7日检索了CENTRAL、MEDLINE、Embase和CINAHL,于2019年11月8日检索了虚拟健康图书馆,于2018年12月5日检索了Popline,于2019年3月22日检索了其他三个数据库,并于2019年11月8日检索了两个试验注册库。我们进行了参考文献核对和引文检索,并联系研究作者以识别其他研究。
随机对照试验(RCT)、整群RCT、前后对照研究(CBA)、中断时间序列(ITS)研究和重复测量研究,比较通用的WHO/UNICEF iCCM(或其本地适应性)针对至少两种iCCM疾病与常规机构服务(机构治疗服务),有无单一疾病社区病例管理(CCM)。我们纳入了报告中低收入国家五岁以下儿童获得适当提供者进行的儿童疾病适当治疗的覆盖率、医疗质量、医疗机构的病例负担或疾病严重程度、死亡率、不良事件以及寻求治疗的覆盖率的研究。
至少两名综述作者独立筛选摘要、筛选全文并使用从EPOC良好实践数据收集表改编的标准化数据收集表提取数据。我们通过讨论解决任何分歧,如有必要,我们会咨询未参与原始筛选的第三位综述作者。必要时,我们联系研究作者以获取澄清或更多细节。我们报告了二分结局的风险比(RR)和事件发生时间结局的风险比(HR),并给出95%置信区间(CI),如有可能,对聚类进行调整。我们尽可能使用研究者报告的主要分析中的效应估计值。我们分别分析了随机试验和其他研究类型的效应。我们使用GRADE方法评估证据的确定性。
我们纳入了七项研究,其中三项是整群RCT,四项是CBA。七项研究中有六项在撒哈拉以南非洲地区,一项研究在南亚。七项研究中的iCCM组成部分和投入相当一致,但在培训和部署部分(例如iCCM提供者的薪酬)和系统部分(例如改善信息系统)存在显著差异。与常规机构服务相比,我们不确定iCCM对任何iCCM疾病获得适当提供者进行的适当治疗覆盖率的影响(RR 0.96,95%CI 0.77至1.19;2项CBA研究,5898名儿童;极低确定性证据)。iCCM可能对新生儿死亡率几乎没有影响(HR 1.01,95%CI 0.73至1.28;2项试验,65209名儿童;低确定性证据)。我们不确定iCCM对婴儿死亡率的影响(HR 1.02,95%CI 0.83至1.26;2项试验,60480名儿童;极低确定性证据)和五岁以下儿童死亡率的影响(HR 1.18,95%CI 1.01至1.37;1项试验,4729名儿童;极低确定性证据)。iCCM可能会使任何iCCM疾病寻求适当提供者治疗的覆盖率提高68%(RR 1.68,95%CI 1.24至2.27;2项试验,9853名儿童;中等确定性证据)。没有研究报告此比较的医疗质量、疾病严重程度或不良事件。与常规机构服务加疟疾CCM相比,我们不确定iCCM对任何iCCM疾病获得适当提供者进行的适当治疗覆盖率的影响(极低确定性证据),并且iCCM可能对任何iCCM疾病寻求适当提供者治疗的影响很小或没有影响(RR 1.06,95%CI 0.97至1.17;1项试验,811名儿童;低确定性证据)。没有研究报告此比较的医疗质量、医疗机构的病例负担或疾病严重程度、死亡率或不良事件。
iCCM可能会增加任何iCCM疾病寻求适当提供者治疗的覆盖率。然而,此处提供的证据强调了超越培训和部署,重视iCCM提供者、加强卫生系统和参与社区系统的重要性。