Jin Zhicheng, Chen Li, Zhong Binyan, Zhou Haifeng, Zhu Haidong, Zhou Hai, Song Jingjing, Guo Jinhe, Zhu Xiaoli, Ji Jiansong, Ni Caifang, Teng Gaojun
Center of Interventional Radiology and Vascular Surgery, Department of Radiology, Zhongda Hospital, Medical School, Southeast University, Nanjing 210009, China.
Department of Interventional Radiology, The First Affiliated Hospital of Soochow University, Suzhou, China.
Transl Oncol. 2021 Apr;14(4):101034. doi: 10.1016/j.tranon.2021.101034. Epub 2021 Feb 7.
Due to the high heterogeneity of hepatocellular carcinoma (HCC), patients with non-advanced disease who are unsuitable for initial transarterial chemoembolization (TACE) monotherapy may have the potential to develop extrahepatic spread or vascular invasion. We aimed to develop and independently validate a radiomics-based model for predicting which patients will develop extrahepatic spread or vascular invasion after initial TACE monotherapy (EVIT).
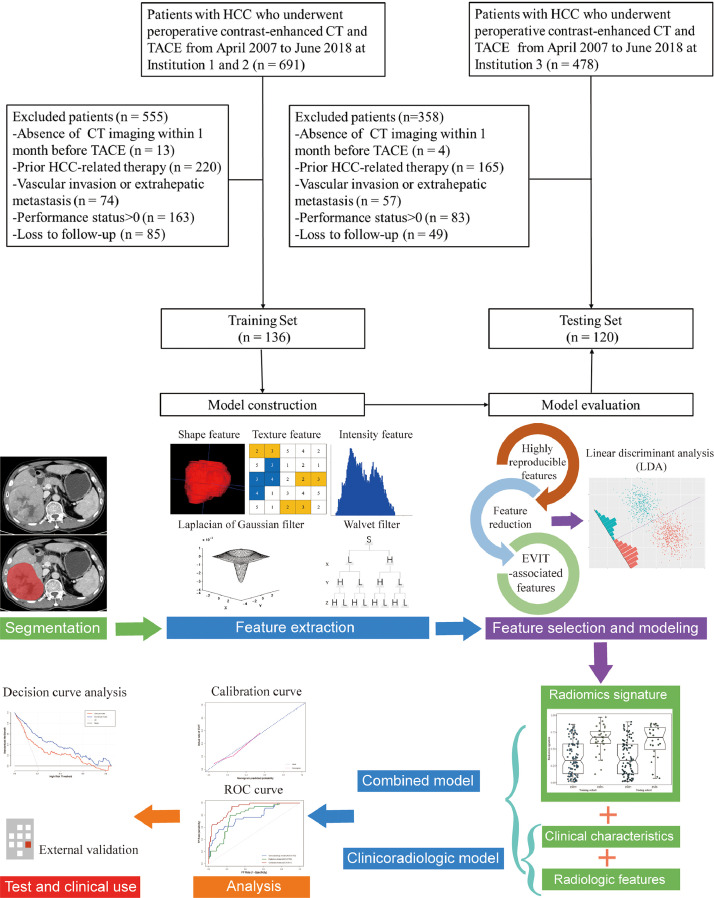
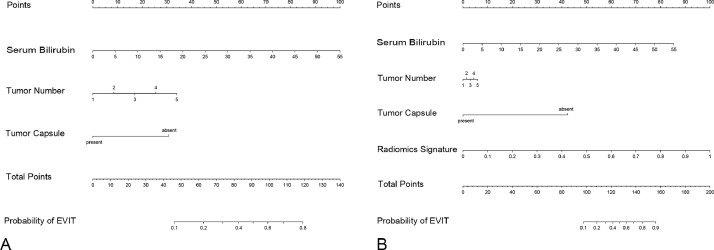
This retrospective study included 256 HCC patients (training set: n = 136; testing set: n = 120) who underwent TACE as initial therapy between April 2007 and June 2018. Clinicoradiological predictors were selected using multivariate logistic regression and a clinicoradiological model was constructed. The radiomic features were extracted from contrast-enhanced computed tomography (CT) images and a radiomics signature was constructed based on a machine learning algorithm. A combined model integrated clinicoradiological predictor and radiomics signature was developed. The predictive performance of the two models was evaluated and compared based on its discrimination, calibration, and clinical usefulness.
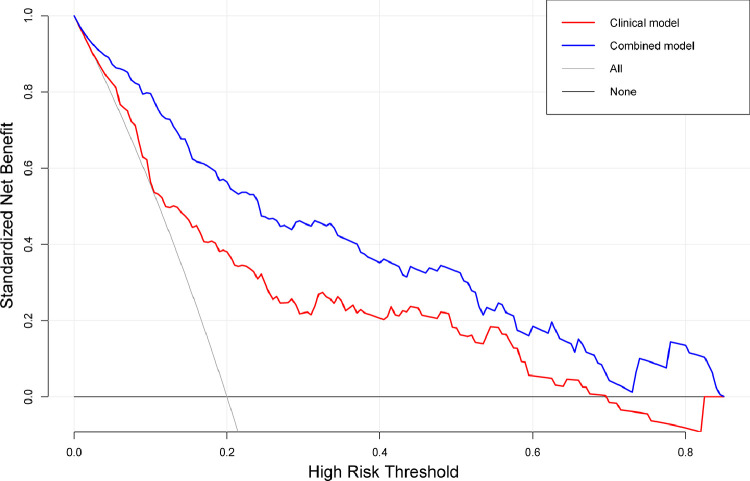
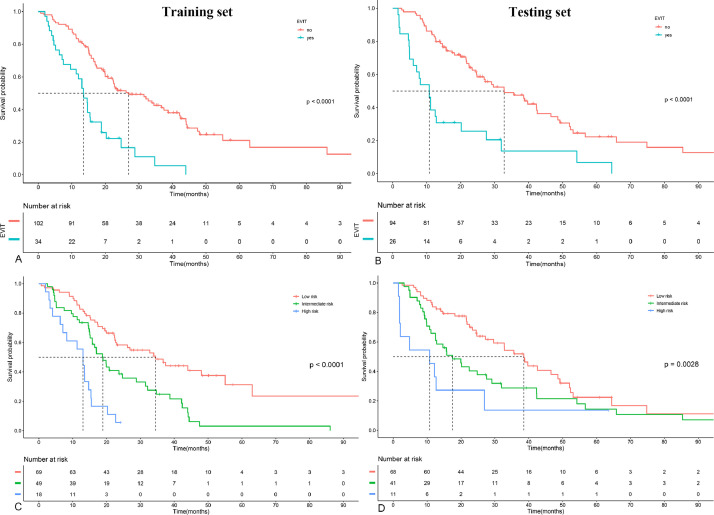
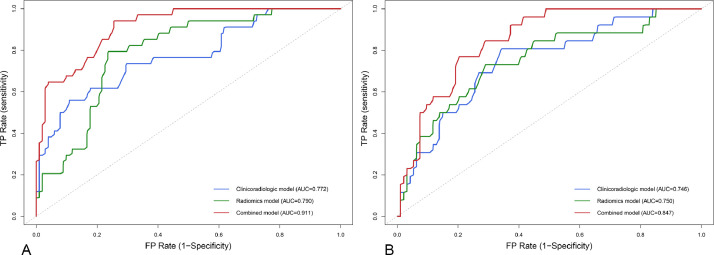
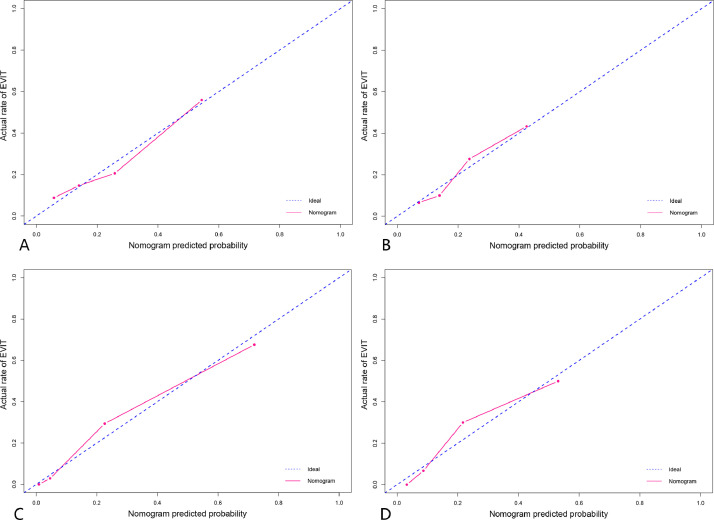
In the training set, 34 (25.0%) patients were confirmed to have EVIT, whereas 26 (21.7%) patients in the testing set had EVIT. When the radiomics signature was added, the combined model showed improved discrimination performance compared to the clinicoradiological model (area under the curves [AUCs] 0.911 vs. 0.772 in the training set; AUCs 0.847 vs. 0.746 in the testing set) and could divide HCC patients into three strata of low, intermediate, or high risk in the two sets. Decision curve analysis demonstrated that the two models were clinically useful, and the combined model provided greater benefits for discriminating patients than the clinicoradiological model.
This study presents a model that integrates clinicoradiological predictors and CT-based radiomics signature that could provide a preoperative individualized prediction of EVIT in patients with HCC.
由于肝细胞癌(HCC)具有高度异质性,不适合初始经动脉化疗栓塞(TACE)单一疗法的非晚期疾病患者可能有发生肝外转移或血管侵犯的风险。我们旨在开发并独立验证一种基于放射组学的模型,以预测哪些患者在初始TACE单一疗法(EVIT)后会发生肝外转移或血管侵犯。
这项回顾性研究纳入了2007年4月至2018年6月期间接受TACE作为初始治疗的256例HCC患者(训练集:n = 136;测试集:n = 120)。使用多变量逻辑回归选择临床放射学预测指标,并构建临床放射学模型。从对比增强计算机断层扫描(CT)图像中提取放射组学特征,并基于机器学习算法构建放射组学特征标签。开发了一个整合临床放射学预测指标和放射组学特征标签的联合模型。基于其区分度、校准度和临床实用性对这两个模型的预测性能进行评估和比较。
在训练集中,34例(25.0%)患者被证实发生EVIT,而测试集中有26例(21.7%)患者发生EVIT。添加放射组学特征标签后,联合模型与临床放射学模型相比,区分性能有所提高(训练集中曲线下面积[AUCs]为0.911对0.772;测试集中AUCs为0.847对0.746),并且可以将HCC患者在两个数据集中分为低、中、高风险三个层次。决策曲线分析表明这两个模型在临床上均有用,并且联合模型在区分患者方面比临床放射学模型具有更大的优势。
本研究提出了一种整合临床放射学预测指标和基于CT的放射组学特征标签的模型,该模型可为HCC患者术前EVIT提供个体化预测。