Africa Health Research Institute, Durban, South Africa.
Lincoln International Institute for Rural Health, University of Lincoln, Lincoln, United Kingdom.
J Int AIDS Soc. 2021 Feb;24(2):e25665. doi: 10.1002/jia2.25665.
The uptake of HIV testing and linkage to care remains low among men, contributing to high HIV incidence in women in South Africa. We conducted the "Home-Based Intervention to Test and Start" (HITS) in a 2x2 factorial cluster randomized controlled trial in one of the World's largest ongoing HIV cohorts in rural South Africa aimed at enhancing both intrinsic and extrinsic motivations for HIV testing.
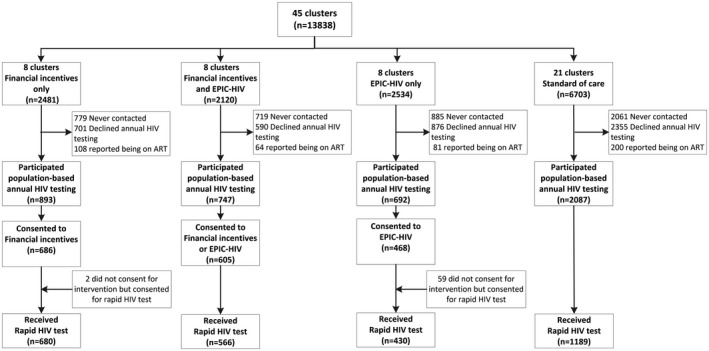
Between February and December 2018, in the uMkhanyakude district of KwaZulu-Natal, we randomly assigned 45 communities (clusters) (n = 13,838 residents) to one of the four arms: (i) financial incentives for home-based HIV testing and linkage to care (R50 [$3] food voucher each); (ii) male-targeted HIV-specific decision support application, called EPIC-HIV; (iii) both financial incentives and male-targeted HIV-specific decision support application and (iv) standard of care (SoC). EPIC-HIV was developed to encourage and serve as an intrinsic motivator for HIV testing and linkage to care, and individually offered to men via a tablet device. Financial incentives were offered to both men and women. Here we report the effect of the interventions on uptake of home-based HIV testing among men. Intention-to-treat (ITT) analysis was performed using modified Poisson regression with adjustment for clustering of standard errors at the cluster levels.
Among all 13,838 men ≥ 15 years living in the 45 communities, the overall population coverage during a single round of home-based HIV testing was 20.7%. The uptake of HIV testing was 27.5% (683/2481) in the financial incentives arm, 17.1% (433/2534) in the EPIC-HIV arm, 26.8% (568/2120) in the arm receiving both interventions and 17.8% in the SoC arm. The probability of HIV testing increased substantially by 55% in the financial incentives arm (risk ratio (RR)=1.55, 95% CI: 1.31 to 1.82, p < 0.001) and 51% in the arm receiving both interventions (RR = 1.51, 95% CI: 1.21 to 1.87 p < 0.001), compared to men in the SoC arm. The probability of HIV testing did not significantly differ in the EPIC-HIV arm (RR = 0.96, 95% CI: 0.76 to 1.20, p = 0.70).
The provision of a small financial incentive acted as a powerful extrinsic motivator substantially increasing the uptake of home-based HIV testing among men in rural South Africa. In contrast, the counselling and testing application which was designed to encourage and serve as an intrinsic motivator to test for HIV did not increase the uptake of home-based testing.
在南非,男性接受 HIV 检测和与医疗保健机构联系的比例仍然很低,这导致了女性 HIV 发病率居高不下。我们在南非农村的一个世界上最大的 HIV 队列中进行了“家庭干预检测和启动”(HITS)的 2x2 析因随机对照试验,旨在增强 HIV 检测的内在和外在动机。
在 2018 年 2 月至 12 月期间,在夸祖鲁-纳塔尔省的 uMkhanyakude 区,我们将 45 个社区(集群)(n=13838 名居民)随机分配到以下四个组之一:(i)家庭 HIV 检测和与医疗保健机构联系的财政激励(每次检测提供 50 兰特[3 美元]的食品券);(ii)针对男性的 HIV 特异性决策支持应用程序,称为 EPIC-HIV;(iii)财政激励和针对男性的 HIV 特异性决策支持应用程序;(iv)标准护理(SoC)。EPIC-HIV 的开发旨在鼓励和作为 HIV 检测和与医疗保健机构联系的内在动机,并通过平板电脑单独提供给男性。财政激励同时提供给男性和女性。在这里,我们报告了这些干预措施对男性家庭 HIV 检测率的影响。采用改良泊松回归进行意向治疗(ITT)分析,并对社区水平的标准误进行聚类调整。
在所有居住在 45 个社区的 13838 名 15 岁及以上的男性中,单次家庭 HIV 检测的总人群覆盖率为 20.7%。HIV 检测的接受率在财政激励组为 27.5%(683/2481),在 EPIC-HIV 组为 17.1%(433/2534),在同时接受两项干预措施的组为 26.8%(568/2120),在 SoC 组为 17.8%。与 SoC 组的男性相比,财政激励组的 HIV 检测概率显著增加了 55%(风险比(RR)=1.55,95%置信区间:1.31 至 1.82,p<0.001),同时接受两项干预措施的组的 HIV 检测概率增加了 51%(RR=1.51,95%置信区间:1.21 至 1.87,p<0.001)。在 EPIC-HIV 组,HIV 检测的概率没有显著差异(RR=0.96,95%置信区间:0.76 至 1.20,p=0.70)。
提供少量财政激励作为一种强大的外在动机,显著增加了南非农村地区男性进行家庭 HIV 检测的比例。相比之下,旨在鼓励和作为 HIV 检测内在动机的咨询和检测应用程序并没有增加家庭检测的比例。