Institute of Biomedical and Clinical Science, University of Exeter College of Medicine and Health, Royal Devon and Exeter Hospital, Exeter EX2 5DW, UK.
BMJ. 2021 Feb 15;372:n214. doi: 10.1136/bmj.n214.
To determine whether the sensitivity and specificity of SNP chips are adequate for detecting rare pathogenic variants in a clinically unselected population.
Retrospective, population based diagnostic evaluation.
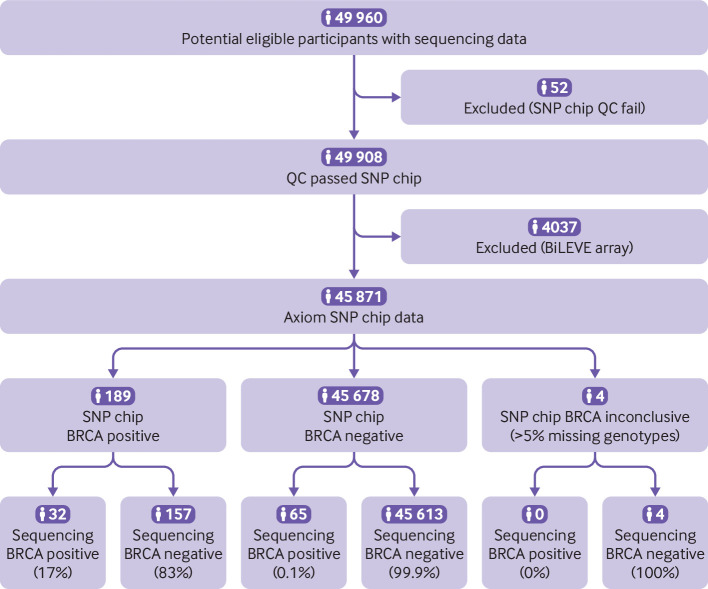
49 908 people recruited to the UK Biobank with SNP chip and next generation sequencing data, and an additional 21 people who purchased consumer genetic tests and shared their data online via the Personal Genome Project.
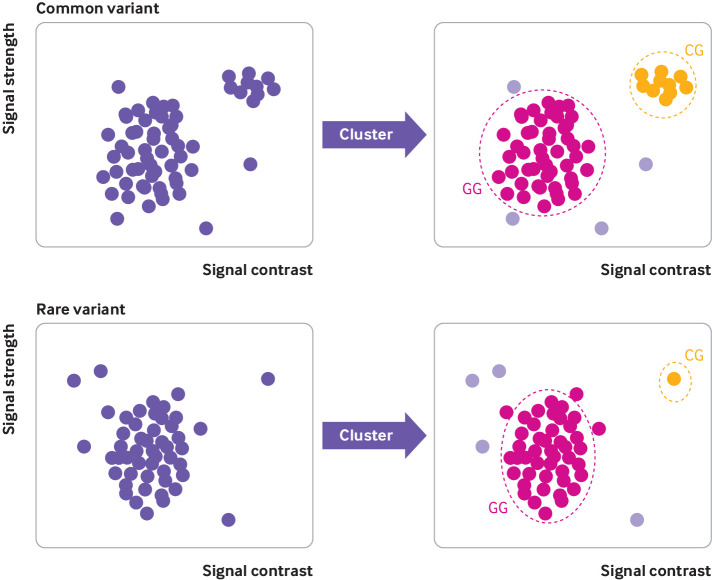
Genotyping (that is, identification of the correct DNA base at a specific genomic location) using SNP chips versus sequencing, with results split by frequency of that genotype in the population. Rare pathogenic variants in the and genes were selected as an exemplar for detailed analysis of clinically actionable variants in the UK Biobank, and BRCA related cancers (breast, ovarian, prostate, and pancreatic) were assessed in participants through use of cancer registry data.
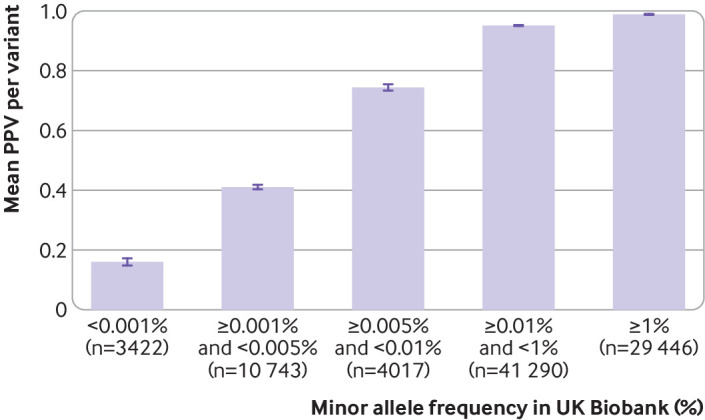
Overall, genotyping using SNP chips performed well compared with sequencing; sensitivity, specificity, positive predictive value, and negative predictive value were all above 99% for 108 574 common variants directly genotyped on the SNP chips and sequenced in the UK Biobank. However, the likelihood of a true positive result decreased dramatically with decreasing variant frequency; for variants that are very rare in the population, with a frequency below 0.001% in UK Biobank, the positive predictive value was very low and only 16% of 4757 heterozygous genotypes from the SNP chips were confirmed with sequencing data. Results were similar for SNP chip data from the Personal Genome Project, and 20/21 individuals analysed had at least one false positive rare pathogenic variant that had been incorrectly genotyped. For pathogenic variants in the and genes, which are individually very rare, the overall performance metrics for the SNP chips versus sequencing in the UK Biobank were: sensitivity 34.6%, specificity 98.3%, positive predictive value 4.2%, and negative predictive value 99.9%. Rates of BRCA related cancers in UK Biobank participants with a positive SNP chip result were similar to those for age matched controls (odds ratio 1.31, 95% confidence interval 0.99 to 1.71) because the vast majority of variants were false positives, whereas sequence positive participants had a significantly increased risk (odds ratio 4.05, 2.72 to 6.03).
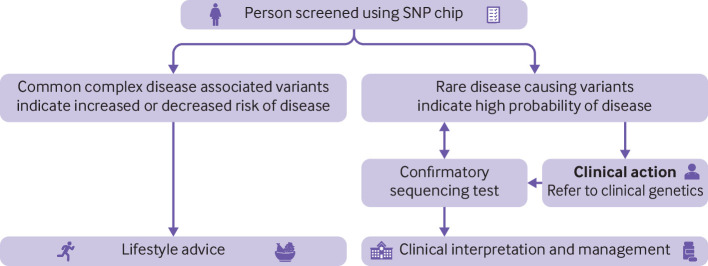
SNP chips are extremely unreliable for genotyping very rare pathogenic variants and should not be used to guide health decisions without validation.
确定 SNP 芯片的灵敏度和特异性是否足以检测临床未选择人群中的罕见致病性变异。
回顾性、基于人群的诊断评估。
49908 人参加了英国生物库的 SNP 芯片和下一代测序数据招募,另外 21 人购买了消费者基因检测,并通过个人基因组计划在线共享他们的数据。
使用 SNP 芯片进行基因分型(即鉴定特定基因组位置的正确 DNA 碱基)与测序结果,结果按该基因型在人群中的频率进行划分。选择 和 基因中的罕见致病性变异作为英国生物库中临床可操作变异详细分析的范例,并通过使用癌症登记数据评估参与者中的 BRCA 相关癌症(乳腺癌、卵巢癌、前列腺癌和胰腺癌)。
总体而言,SNP 芯片的基因分型与测序相比表现良好;直接在 SNP 芯片上进行基因分型并在英国生物库中测序的 108574 个常见变异的敏感性、特异性、阳性预测值和阴性预测值均高于 99%。然而,真阳性结果的可能性随着变异频率的降低而急剧下降;对于在人群中非常罕见的变异,在英国生物库中的频率低于 0.001%,阳性预测值非常低,并且 SNP 芯片上的 4757 个杂合基因型中只有 16%得到测序数据的确认。来自个人基因组计划的 SNP 芯片数据的结果相似,分析的 20/21 个人至少有一个错误地进行基因分型的罕见致病性假阳性变异。对于 基因和 基因中的致病性变异,每个基因都非常罕见,SNP 芯片与测序在英国生物库中的总体性能指标为:敏感性 34.6%,特异性 98.3%,阳性预测值 4.2%,阴性预测值 99.9%。在 SNP 芯片结果阳性的英国生物库参与者中,BRCA 相关癌症的发病率与年龄匹配的对照组相似(比值比 1.31,95%置信区间 0.99 至 1.71),因为绝大多数变异都是假阳性,而序列阳性参与者的风险显著增加(比值比 4.05,2.72 至 6.03)。
SNP 芯片极不可靠,无法对非常罕见的致病性变异进行基因分型,在未经验证的情况下,不应用于指导健康决策。