Nkurunungi Gyaviira, Zirimenya Ludoviko, Natukunda Agnes, Nassuuna Jacent, Oduru Gloria, Ninsiima Caroline, Zziwa Christopher, Akello Florence, Kizindo Robert, Akello Mirriam, Kaleebu Pontiano, Wajja Anne, Luzze Henry, Cose Stephen, Webb Emily, Elliott Alison M
Immunomodulation and Vaccines Programme, Medical Research Council/Uganda Virus Research Institute and London School of Hygiene and Tropical Medicine (MRC/UVRI and LSHTM) Uganda Research Unit, Entebbe, Uganda
Immunomodulation and Vaccines Programme, Medical Research Council/Uganda Virus Research Institute and London School of Hygiene and Tropical Medicine (MRC/UVRI and LSHTM) Uganda Research Unit, Entebbe, Uganda.
BMJ Open. 2021 Feb 16;11(2):e040425. doi: 10.1136/bmjopen-2020-040425.
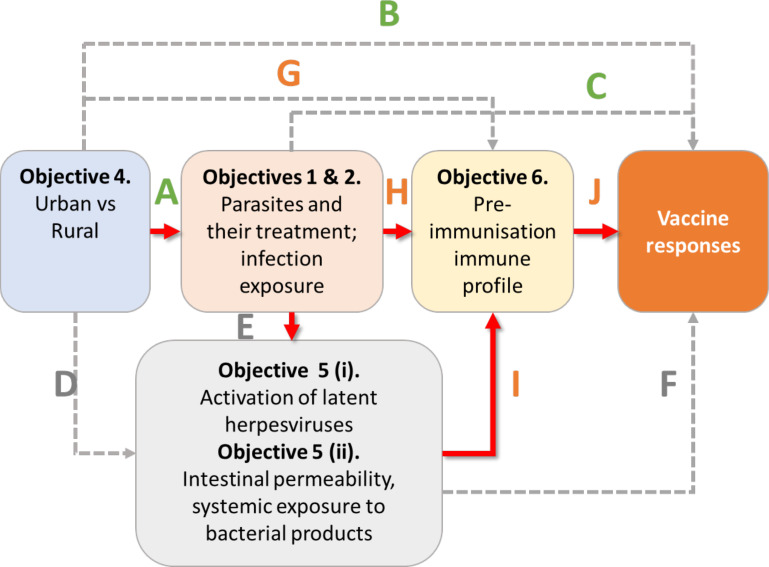
Vaccine-specific immune responses vary between populations and are often impaired in low income, rural settings. Drivers of these differences are not fully elucidated, hampering identification of strategies for optimising vaccine effectiveness. We hypothesise that urban-rural (and regional and international) differences in vaccine responses are mediated to an important extent by differential exposure to chronic infections, particularly parasitic infections.
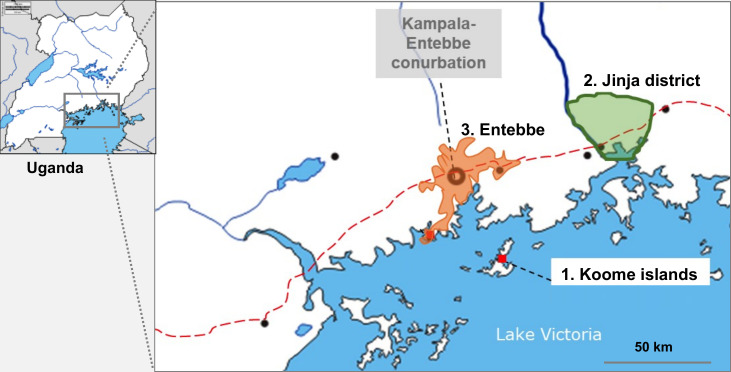
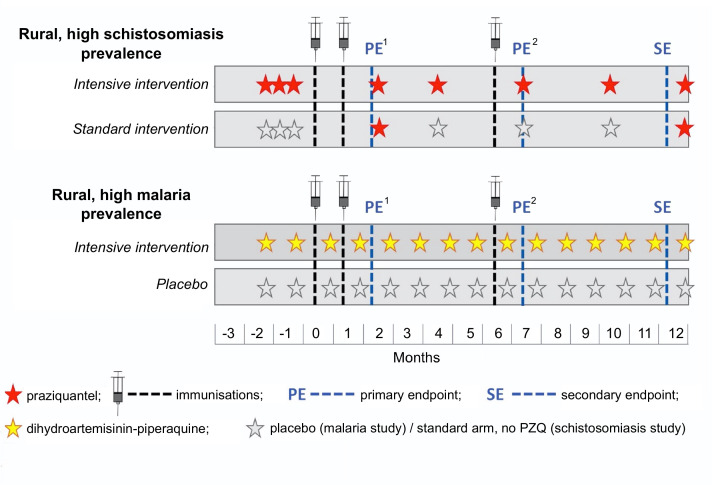
Three related trials sharing core elements of study design and procedures (allowing comparison of outcomes across the trials) will test the effects of (1) individually randomised intervention against schistosomiasis (trial A) and malaria (trial B), and (2) Bacillus Calmette-Guérin (BCG) revaccination (trial C), on a common set of vaccine responses. We will enrol adolescents from Ugandan schools in rural high-schistosomiasis (trial A) and rural high-malaria (trial B) settings and from an established urban birth cohort (trial C). All participants will receive BCG on day '0'; yellow fever, oral typhoid and human papilloma virus (HPV) vaccines at week 4; and HPV and tetanus/diphtheria booster vaccine at week 28. Primary outcomes are BCG-specific IFN-γ responses (8 weeks after BCG) and for other vaccines, antibody responses to key vaccine antigens at 4 weeks after immunisation. Secondary analyses will determine effects of interventions on correlates of protective immunity, vaccine response waning, priming versus boosting immunisations, and parasite infection status and intensity. Overarching analyses will compare outcomes between the three trial settings. Sample archives will offer opportunities for exploratory evaluation of the role of immunological and 'trans-kingdom' mediators in parasite modulation of vaccine-specific responses.
Ethics approval has been obtained from relevant Ugandan and UK ethics committees. Results will be shared with Uganda Ministry of Health, relevant district councils, community leaders and study participants. Further dissemination will be done through conference proceedings and publications.
ISRCTN60517191, ISRCTN62041885, ISRCTN10482904.
疫苗特异性免疫反应在不同人群中存在差异,在低收入农村地区往往受损。这些差异的驱动因素尚未完全阐明,这妨碍了优化疫苗效力策略的确定。我们假设,疫苗反应的城乡(以及地区和国际)差异在很大程度上是由对慢性感染,尤其是寄生虫感染的不同暴露介导的。
三项具有共同研究设计和程序核心要素(允许比较各试验结果)的相关试验将测试以下因素的影响:(1)针对血吸虫病(试验A)和疟疾(试验B)的个体随机干预,以及(2)卡介苗(BCG)再接种(试验C),对一组共同的疫苗反应的影响。我们将招募来自乌干达农村血吸虫病高发地区(试验A)和农村疟疾高发地区(试验B)学校的青少年,以及来自一个既定城市出生队列(试验C)的青少年。所有参与者将在第0天接种卡介苗;在第4周接种黄热病、口服伤寒和人乳头瘤病毒(HPV)疫苗;在第28周接种HPV和破伤风/白喉加强疫苗。主要结局是卡介苗特异性干扰素-γ反应(卡介苗接种后8周),对于其他疫苗,是免疫接种后4周对关键疫苗抗原的抗体反应。二次分析将确定干预措施对保护性免疫相关因素、疫苗反应减弱、初次免疫与加强免疫以及寄生虫感染状态和强度的影响。总体分析将比较三个试验地点的结果。样本存档将为探索性评估免疫和“跨界”介质在寄生虫对疫苗特异性反应调节中的作用提供机会。
已获得乌干达和英国相关伦理委员会的伦理批准。结果将与乌干达卫生部、相关地区委员会、社区领袖和研究参与者分享。进一步的传播将通过会议论文集和出版物进行。
ISRCTN60517191、ISRCTN62041885、ISRCTN10482904。