Rheumatology Unit, Department of Medical Sciences and Public Health, AOU University Clinic and University of Cagliari, SS 554, 09042, Monserrato, CA, Italy.
BioDrugs. 2021 Mar;35(2):175-186. doi: 10.1007/s40259-021-00467-w. Epub 2021 Feb 17.
Our objective was to update the understanding of the development of paradoxical immune-mediated glomerular disorders (IGDs) in patients with rheumatic diseases treated with biologics and targeted synthetic drugs (ts-drugs).
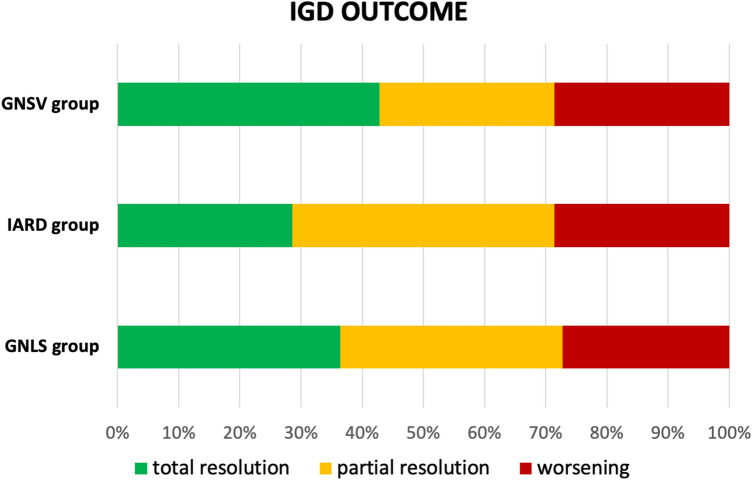
A systematic literature review was performed by searching PubMed for articles published between 1 January 2014 and 1 January 2020 reporting on the development of IGD in adult patients with rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis or systemic lupus erythematosus (SLE) who were receiving biologics or ts-drugs. IGDs were classified on the basis of clinical, laboratory and histopathological data as (1) glomerulonephritis associated with systemic vasculitis (GNSV), (2) isolated autoimmune renal disorder (IARD) or (3) glomerulonephritis in SLE and in lupus-like syndrome (GNLS). The World Health Organization-Uppsala Monitoring Centre (WHO-UMC) system for standardized case causality assessment was applied to evaluate the causal relationship between IGD and specific drugs. The classification was based on a six-category scale, where the "certain" and "probable" categories were deemed clinically relevant relationships.
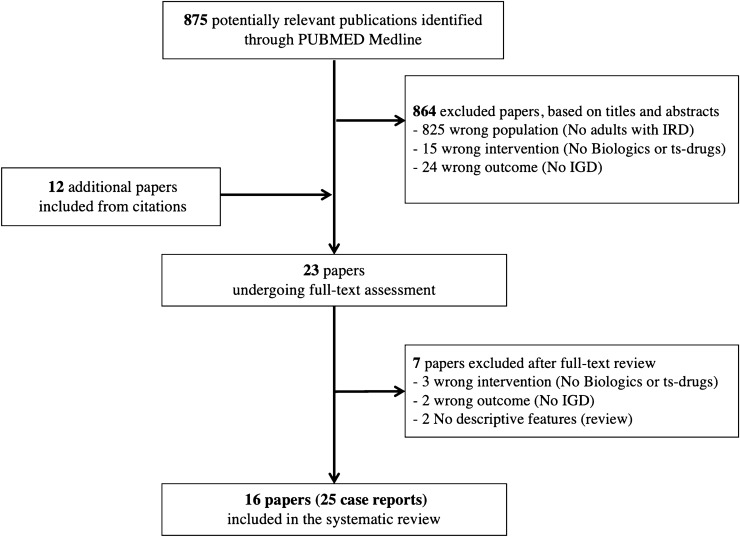
The literature search retrieved 875 articles. Of these, 16 articles reported IGD data, for a total of 25 cases. According to the WHO-UMC assessment, the strength of the causal relationship between IGDs and investigated drugs was higher for anti-tumor necrosis factor-α agents (a clinically relevant relationship was found in four of six cases), abatacept (one of two cases), tocilizumab (two cases), ustekinumab (one case) and tofacitinib (one case) than for rituximab (nine cases), belimumab (three cases) or secukinumab (one case), which showed a weak causal relationship with these paradoxical events. No cases associated with apremilast or baricitinib were found. The retrieved cases were classified as 11 GNLS, seven IARD and seven GNSV.
Biologics and ts-drugs can cause IGDs. These events are rare, and the causative effect of a specific drug is hard to establish. When a patient is suspected of having an IGD, the drug should be discontinued, and treatment for the new-onset renal disorder should be promptly started.
本研究旨在更新对接受生物制剂和靶向合成药物(ts-drugs)治疗的风湿性疾病患者发生免疫介导的矛盾性肾小球疾病(IGD)的认识。
通过在 PubMed 上检索 2014 年 1 月 1 日至 2020 年 1 月 1 日期间发表的报告类风湿关节炎、银屑病关节炎、强直性脊柱炎或系统性红斑狼疮(SLE)成年患者在接受生物制剂或 ts-drugs 治疗期间发生 IGD 的文章,进行系统文献回顾。根据临床、实验室和组织病理学数据,将 IGD 分为(1)与系统性血管炎相关的肾小球肾炎(GNSV),(2)孤立性自身免疫性肾脏疾病(IARD)或(3)SLE 和狼疮样综合征中的肾小球肾炎(GNLS)。应用世界卫生组织-乌普萨拉监测中心(WHO-UMC)系统对标准化病例因果关系评估来评估 IGD 与特定药物之间的因果关系。分类基于六级量表,其中“确定”和“可能”类别被认为与临床相关。
文献检索共检索到 875 篇文章,其中 16 篇文章报告了 IGD 数据,共 25 例。根据 WHO-UMC 评估,抗 TNF-α 制剂(在 6 例中有 4 例发现具有临床相关关系)、阿巴西普(2 例中有 1 例)、托珠单抗(2 例)、乌司奴单抗(1 例)和托法替布(1 例)与 IGD 之间的因果关系强度更高,而利妥昔单抗(9 例)、贝利尤单抗(3 例)或司库奇尤单抗(1 例)与这些矛盾事件的因果关系较弱。未发现与阿普米司特或巴瑞替尼相关的病例。检索到的病例分为 11 例 GNLS、7 例 IARD 和 7 例 GNSV。
生物制剂和 ts-drugs 可引起 IGD。这些事件罕见,且很难确定特定药物的因果作用。当怀疑患者发生 IGD 时,应停用药物,并及时开始治疗新出现的肾脏疾病。