Bendavid Eran, Mulaney Bianca, Sood Neeraj, Shah Soleil, Bromley-Dulfano Rebecca, Lai Cara, Weissberg Zoe, Saavedra-Walker Rodrigo, Tedrow Jim, Bogan Andrew, Kupiec Thomas, Eichner Daniel, Gupta Ribhav, Ioannidis John P A, Bhattacharya Jay
Department of Medicine, Stanford University School of Medicine, Stanford, CA, USA.
Stanford University School of Medicine, Stanford, CA, USA.
Int J Epidemiol. 2021 May 17;50(2):410-419. doi: 10.1093/ije/dyab010.
Measuring the seroprevalence of antibodies to Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is central to understanding infection risk and fatality rates. We studied Coronavirus Disease 2019 (COVID-19)-antibody seroprevalence in a community sample drawn from Santa Clara County.
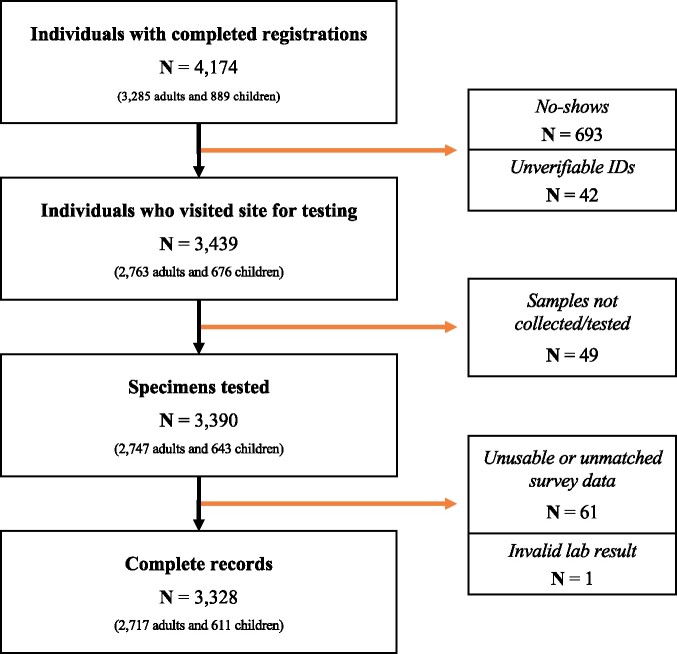
On 3 and 4 April 2020, we tested 3328 county residents for immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies to SARS-CoV-2 using a rapid lateral-flow assay (Premier Biotech). Participants were recruited using advertisements that were targeted to reach county residents that matched the county population by gender, race/ethnicity and zip code of residence. We estimate weights to match our sample to the county by zip, age, sex and race/ethnicity. We report the weighted and unweighted prevalence of antibodies to SARS-CoV-2. We adjust for test-performance characteristics by combining data from 18 independent test-kit assessments: 14 for specificity and 4 for sensitivity.
The raw prevalence of antibodies in our sample was 1.5% [exact binomial 95% confidence interval (CI) 1.1-2.0%]. Test-performance specificity in our data was 99.5% (95% CI 99.2-99.7%) and sensitivity was 82.8% (95% CI 76.0-88.4%). The unweighted prevalence adjusted for test-performance characteristics was 1.2% (95% CI 0.7-1.8%). After weighting for population demographics, the prevalence was 2.8% (95% CI 1.3-4.2%), using bootstrap to estimate confidence bounds. These prevalence point estimates imply that 53 000 [95% CI 26 000 to 82 000 using weighted prevalence; 23 000 (95% CI 14 000-35 000) using unweighted prevalence] people were infected in Santa Clara County by late March-many more than the ∼1200 confirmed cases at the time.
The estimated prevalence of SARS-CoV-2 antibodies in Santa Clara County implies that COVID-19 was likely more widespread than indicated by the number of cases in late March, 2020. At the time, low-burden contexts such as Santa Clara County were far from herd-immunity thresholds.
测量严重急性呼吸综合征冠状病毒2(SARS-CoV-2)抗体的血清流行率对于了解感染风险和死亡率至关重要。我们对从圣克拉拉县抽取的社区样本中的2019冠状病毒病(COVID-19)抗体血清流行率进行了研究。
2020年4月3日和4日,我们使用快速侧向流动检测法(普瑞米尔生物技术公司)对3328名县居民进行了SARS-CoV-2免疫球蛋白G(IgG)和免疫球蛋白M(IgM)抗体检测。通过针对性广告招募参与者,目标是招募在性别、种族/族裔和居住邮政编码方面与县人口匹配的县居民。我们估计权重,以使我们的样本在邮政编码、年龄、性别和种族/族裔方面与该县相匹配。我们报告了SARS-CoV-2抗体的加权和未加权流行率。通过合并来自18项独立检测试剂盒评估的数据来调整检测性能特征:14项用于特异性,4项用于敏感性。
我们样本中抗体的原始流行率为1.5%[精确二项式95%置信区间(CI)1.1 - 2.0%]。我们数据中的检测性能特异性为99.5%(95%CI 99.2 - 99.7%),敏感性为82.8%(95%CI 76.0 - 88.4%)。经检测性能特征调整后的未加权流行率为1.2%(95%CI 0.7 - 1.8%)。在根据人口统计学进行加权后,使用自助法估计置信区间,流行率为2.8%(95%CI 1.3 - 4.2%)。这些流行率点估计表明,到3月下旬,圣克拉拉县有53000人[使用加权流行率时95%CI为26000至82000;使用未加权流行率时为23000(95%CI 14000 - 35000)]感染,远多于当时约1200例确诊病例。
圣克拉拉县SARS-CoV-2抗体的估计流行率表明,COVID-19的实际传播范围可能比2020年3月下旬的病例数所显示的更广。当时,像圣克拉拉县这样负担较轻的地区远未达到群体免疫阈值。