Department of Pharmacy, Radboud Institute for Health Sciences, Radboud University Medical Center, Geert Grooteplein zuid 10, 864, 6500 HB, Nijmegen, The Netherlands.
School of Pharmacy, Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia.
Clin Pharmacokinet. 2021 Jul;60(7):943-953. doi: 10.1007/s40262-020-00971-2. Epub 2021 Feb 22.
This study aimed to develop and evaluate a population pharmacokinetic model and limited sampling strategy for isoniazid to be used in model-based therapeutic drug monitoring.
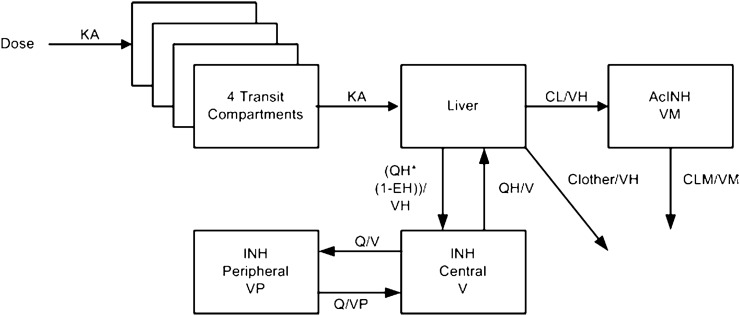
A population pharmacokinetic model was developed based on isoniazid and acetyl-isoniazid pharmacokinetic data from seven studies with in total 466 patients from three continents. Three limited sampling strategies were tested based on the available sampling times in the dataset and practical considerations. The tested limited sampling strategies sampled at 2, 4, and 6 h, 2 and 4 h, and 2 h after dosing. The model-predicted area under the concentration-time curve from 0 to 24 h (AUC) and the peak concentration from the limited sampling strategies were compared to predictions using the full pharmacokinetic curve. Bias and precision were assessed using the mean error (ME) and the root mean square error (RMSE), both expressed as a percentage of the mean model-predicted AUC or peak concentration on the full pharmacokinetic curve.
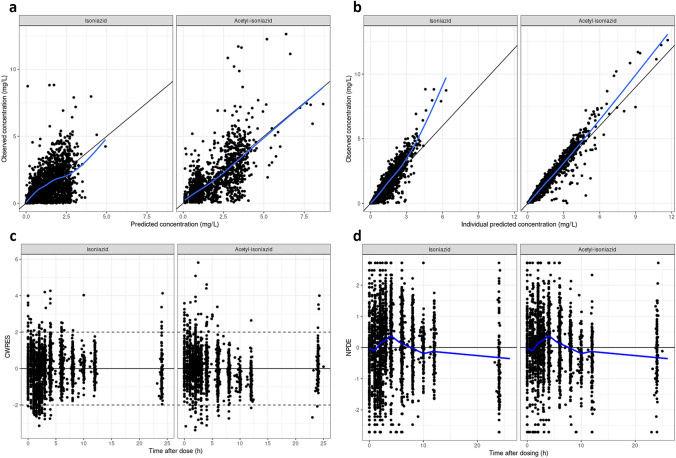
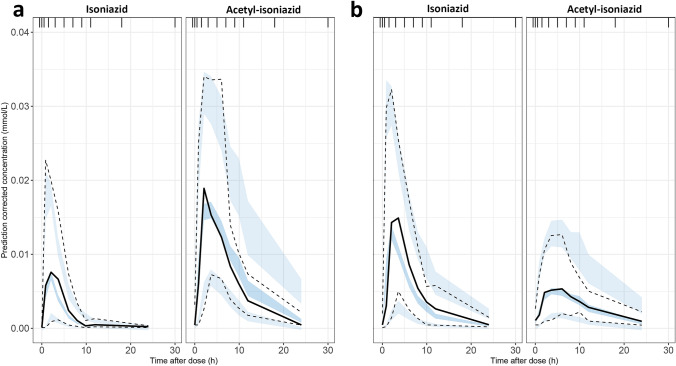
Performance of the developed model was acceptable and the uncertainty in parameter estimations was generally low (the highest relative standard error was 39% coefficient of variation). The limited sampling strategy with sampling at 2 and 4 h was determined as most suitable with an ME of 1.1% and RMSE of 23.4% for AUC prediction, and ME of 2.7% and RMSE of 23.8% for peak concentration prediction. For the performance of this strategy, it is important that data on both isoniazid and acetyl-isoniazid are used. If only data on isoniazid are available, a limited sampling strategy using 2, 4, and 6 h can be employed with an ME of 1.7% and RMSE of 20.9% for AUC prediction, and ME of 1.2% and RMSE of 23.8% for peak concentration prediction.
A model-based therapeutic drug monitoring strategy for personalized dosing of isoniazid using sampling at 2 and 4 h after dosing was successfully developed. Prospective evaluation of this strategy will show how it performs in a clinical therapeutic drug monitoring setting.
本研究旨在开发并评估异烟肼群体药代动力学模型和基于模型的治疗药物监测的有限采样策略。
基于来自三大洲的 7 项研究中 466 例患者的异烟肼和乙酰异烟肼药代动力学数据,建立了群体药代动力学模型。根据数据集中的可用采样时间和实际考虑,测试了 3 种有限采样策略。所测试的有限采样策略在给药后 2、4 和 6 小时,2 和 4 小时以及 2 小时采样。比较了有限采样策略模型预测的 0 至 24 小时(AUC)和峰浓度与使用全药代动力学曲线的预测结果。使用平均误差(ME)和均方根误差(RMSE)评估偏差和精度,两者均表示为全药代动力学曲线模型预测 AUC 或峰浓度的百分比。
所开发模型的性能可接受,参数估计的不确定性通常较低(最高相对标准误差为 39%变异系数)。采样时间为 2 和 4 小时的有限采样策略被确定为最适合的策略,AUC 预测的 ME 为 1.1%,RMSE 为 23.4%,峰浓度预测的 ME 为 2.7%,RMSE 为 23.8%。对于该策略的性能,重要的是使用异烟肼和乙酰异烟肼的数据。如果仅获得异烟肼的数据,则可以使用采样时间为 2、4 和 6 小时的有限采样策略,AUC 预测的 ME 为 1.7%,RMSE 为 20.9%,峰浓度预测的 ME 为 1.2%,RMSE 为 23.8%。
成功开发了一种基于模型的治疗药物监测策略,用于根据给药后 2 和 4 小时的采样对异烟肼进行个体化给药。该策略的前瞻性评估将展示其在临床治疗药物监测环境中的表现。