Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University, Baltimore, Maryland.
Department of Pharmacy, The Johns Hopkins Hospital, Baltimore, Maryland.
JAMA Netw Open. 2021 Feb 1;4(2):e2037632. doi: 10.1001/jamanetworkopen.2020.37632.
Improved survival in patients with advanced cancer has increased the need for better understanding of how to manage common symptoms that they may experience, such as breathlessness.
To assess the benefits and harms associated with pharmacologic interventions for breathlessness in adults with advanced cancer.
PubMed, Embase, CINAHL, Web of Science, and the Cochrane Central Register of Controlled Trials were searched for studies published from database inception through May 31, 2020, using predefined eligibility criteria within a PICOTS (population, intervention, comparator, outcome, timing, setting) format.
Randomized clinical trials (RCTs), non-RCTs, and observational studies with a comparison group that evaluated benefits and/or harms and cohort studies that reported harms were selected.
Two reviewers independently screened studies for eligibility, serially abstracted data, independently assessed risk of bias, and graded strength of evidence (SOE).
Benefits and harms of pharmacologic interventions were compared, focusing on breathlessness, anxiety, exercise capacity, and health-related quality of life. When possible, meta-analyses were conducted and standardized mean differences (SMDs) calculated.
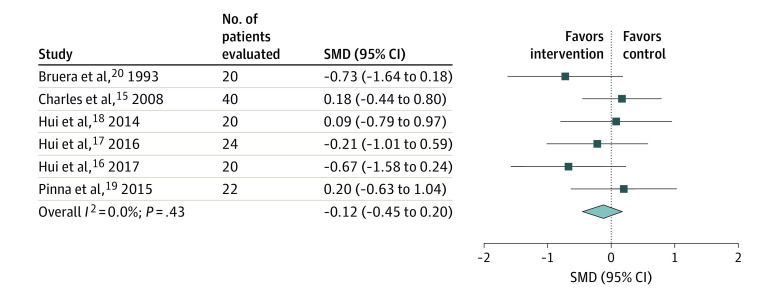
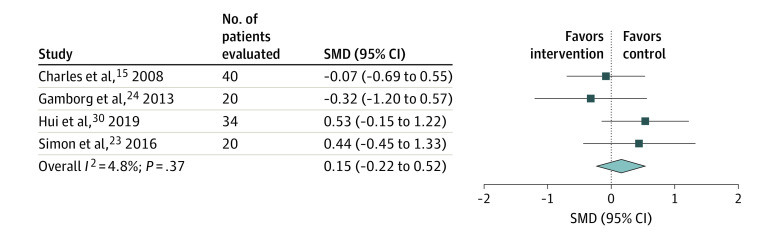
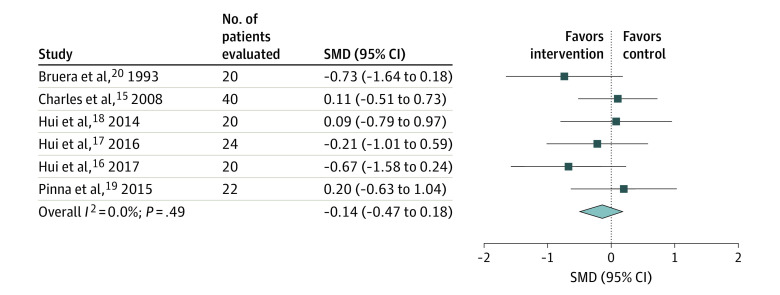
In this systematic review and meta-analysis, a total of 7729 unique citations were identified, of which 19 studies (17 RCTs and 2 retrospective studies) that included a total of 1424 patients assessed the benefits of medications for management of breathlessness in advanced cancer or reported harms. The most commonly reported type of cancer was lung cancer. Opioids were not associated with more effectiveness than placebo for improving breathlessness (SMD, -0.14; 95% CI, -0.47 to 0.18) or exercise capacity ( SMD, 0.06; 95% CI, -0.43 to 0.55) (SOE, moderate); most studies examined exertional breathlessness. Specific dose and/or route of administration of opioids did not differ in effectiveness for breathlessness (SMD, 0.15; 95% CI, -0.22 to 0.52) (SOE, low). Anxiolytics were not associated with more effectiveness than placebo for breathlessness or anxiety (reported mean between-group difference, -0.52; 95% CI, -1.045 to 0.005) (SOE, low). Evidence for other pharmacologic interventions was limited. Pharmacologic interventions demonstrated some harms compared with usual care, but dropout attributable to adverse events was minimal in these short-term studies (range 3.2%-16%).
Evidence did not support the association of opioids or other pharmacologic interventions with improved breathlessness. Given that studies had many limitations, pharmacologic interventions should be considered in selected patients but need to be considered in the context of potential harms and evidence of an association of nonpharmacologic interventions with improved breathlessness.
晚期癌症患者的生存率提高,增加了人们对如何更好地管理他们可能经历的常见症状(如呼吸困难)的理解的需求。
评估在晚期癌症成人中,药物干预呼吸困难的益处和危害。
通过预定义的 PICOTS(人群、干预、比较、结局、时间、地点)格式,在 PubMed、Embase、CINAHL、Web of Science 和 Cochrane 对照试验中心注册库中检索从数据库建立开始到 2020 年 5 月 31 日发表的研究,进行研究选择。
选择了随机临床试验(RCT)、非 RCT 和具有比较组的观察性研究,评估了益处和/或危害,以及报告危害的队列研究。
两名审查员独立筛选研究的资格,连续提取数据,独立评估偏倚风险,并对证据强度(SOE)进行分级。
比较了药物干预的益处和危害,重点是呼吸困难、焦虑、运动能力和健康相关生活质量。在可能的情况下,进行了荟萃分析并计算了标准化均数差(SMD)。
在这项系统评价和荟萃分析中,共确定了 7729 个独特的引文,其中 19 项研究(17 项 RCT 和 2 项回顾性研究)共纳入了 1424 名患者,评估了药物治疗晚期癌症呼吸困难的益处或报告了危害。报告的最常见癌症类型是肺癌。与安慰剂相比,阿片类药物并没有更有效地改善呼吸困难(SMD,-0.14;95%CI,-0.47 至 0.18)或运动能力(SMD,0.06;95%CI,-0.43 至 0.55)(SOE,中等);大多数研究检查了运动性呼吸困难。阿片类药物的特定剂量和/或给药途径在呼吸困难方面的疗效没有差异(SMD,0.15;95%CI,-0.22 至 0.52)(SOE,低)。与安慰剂相比,抗焦虑药并没有更有效地改善呼吸困难或焦虑(报告的组间差异均值为-0.52;95%CI,-1.045 至 0.005)(SOE,低)。其他药物干预的证据有限。与常规护理相比,药物干预确实显示出一些危害,但这些短期研究中因不良反应而导致的辍学率很低(范围为 3.2%-16%)。
证据不支持阿片类药物或其他药物干预与改善呼吸困难之间的关联。鉴于研究存在诸多局限性,应考虑在选定患者中使用药物干预,但需要考虑到潜在危害,并考虑非药物干预与改善呼吸困难之间的关联的证据。