From Baylor College of Medicine, Houston (I.O.R.); James J. Peters Veterans Affairs Medical Center, Bronx, and Icahn School of Medicine at Mount Sinai, New York - both in New York (N.B.); eStudy Site, Chula Vista (M.W.), Genentech, South San Francisco (M.B., L.T.), and the University of California, San Diego, La Jolla (A.M.) - all in California; Hackensack Meridian School of Medicine and Hacksensack University Medical Center, Hackensack, NJ (R.C.G.); Intermountain Healthcare, Salt Lake City (B.D.H.); Royal Free Hospital (S.B.) and Imperial College London (N.C., T.Y.), London, Leeds Teaching Hospitals NHS Trust and National Institute for Health Research-Leeds Biomedical Research Centre, Leeds (S.S.), North Manchester General Hospital, Manchester (A.U.), and Roche Products, Welwyn Garden City (S.D., E.G., B.M., H.S.) - all in the United Kingdom; the University of Massachusetts Medical School-Baystate, Springfield (D.S.); Rush University Medical Center, Chicago (M.S.A.); Denver Health Medical Center, Denver (I.S.D.), and the University of Colorado, Anschutz School of Medicine, Aurora (I.S.D.); University Health Network, Toronto (L.D.S.); Hospital Universitario HM Sanchinarro, Centro Integral, Oncológico Clara Campal and Departamento de Ciencias Médicas Clínicas, Facultad de Medicina, Universidad CEU San Pablo, Madrid (A.C.G.); and the University of Miami Miller School of Medicine, Miami (D.J.D.L.Z.).
N Engl J Med. 2021 Apr 22;384(16):1503-1516. doi: 10.1056/NEJMoa2028700. Epub 2021 Feb 25.
Coronavirus disease 2019 (Covid-19) is associated with immune dysregulation and hyperinflammation, including elevated interleukin-6 levels. The use of tocilizumab, a monoclonal antibody against the interleukin-6 receptor, has resulted in better outcomes in patients with severe Covid-19 pneumonia in case reports and retrospective observational cohort studies. Data are needed from randomized, placebo-controlled trials.
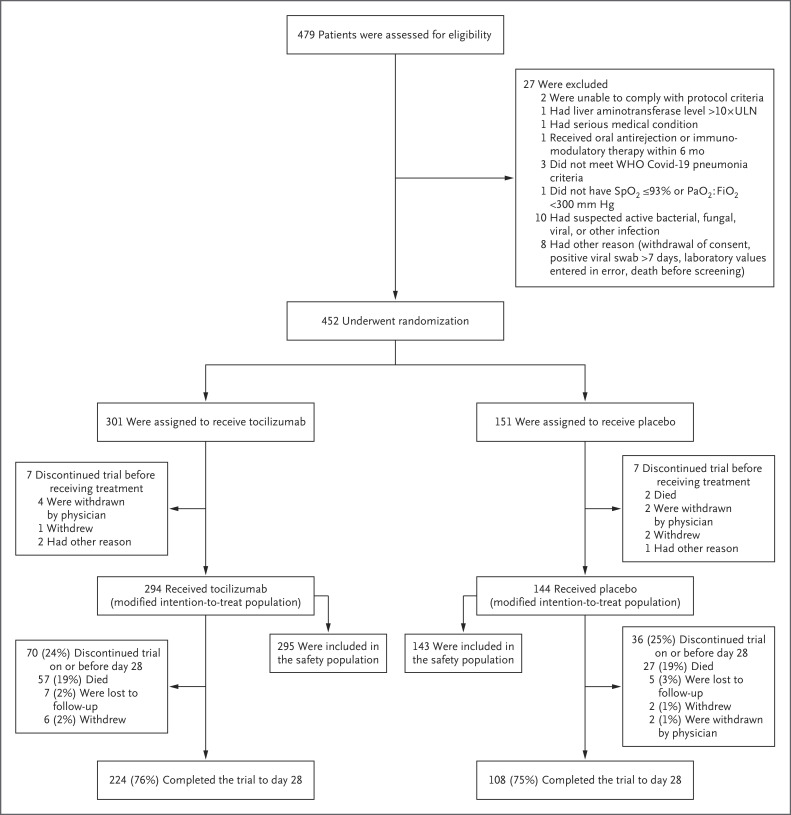
In this phase 3 trial, we randomly assigned patients who were hospitalized with severe Covid-19 pneumonia in a 2:1 ratio receive a single intravenous infusion of tocilizumab (at a dose of 8 mg per kilogram of body weight) or placebo. Approximately one quarter of the participants received a second dose of tocilizumab or placebo 8 to 24 hours after the first dose. The primary outcome was clinical status at day 28 on an ordinal scale ranging from 1 (discharged or ready for discharge) to 7 (death) in the modified intention-to-treat population, which included all the patients who had received at least one dose of tocilizumab or placebo.
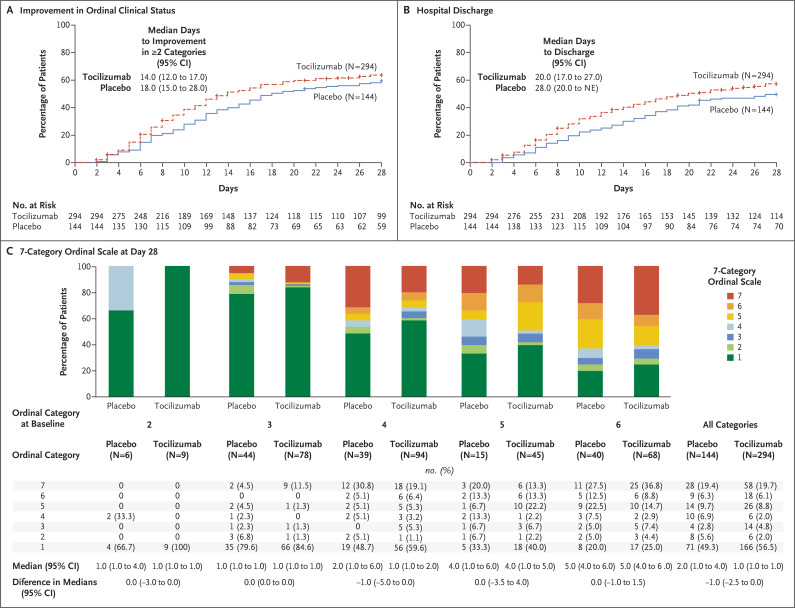
Of the 452 patients who underwent randomization, 438 (294 in the tocilizumab group and 144 in the placebo group) were included in the primary and secondary analyses. The median value for clinical status on the ordinal scale at day 28 was 1.0 (95% confidence interval [CI], 1.0 to 1.0) in the tocilizumab group and 2.0 (non-ICU hospitalization without supplemental oxygen) (95% CI, 1.0 to 4.0) in the placebo group (between-group difference, -1.0; 95% CI, -2.5 to 0; P = 0.31 by the van Elteren test). In the safety population, serious adverse events occurred in 103 of 295 patients (34.9%) in the tocilizumab group and in 55 of 143 patients (38.5%) in the placebo group. Mortality at day 28 was 19.7% in the tocilizumab group and 19.4% in the placebo group (weighted difference, 0.3 percentage points; 95% CI, -7.6 to 8.2; nominal P = 0.94).
In this randomized trial involving hospitalized patients with severe Covid-19 pneumonia, the use of tocilizumab did not result in significantly better clinical status or lower mortality than placebo at 28 days. (Funded by F. Hoffmann-La Roche and the Department of Health and Human Services; COVACTA ClinicalTrials.gov number, NCT04320615.).
2019 年冠状病毒病(COVID-19)与免疫失调和过度炎症有关,包括白细胞介素-6 水平升高。在病例报告和回顾性观察队列研究中,使用针对白细胞介素-6 受体的单克隆抗体托珠单抗可改善重症 COVID-19 肺炎患者的预后。需要来自随机、安慰剂对照试验的数据。
在这项 3 期试验中,我们以 2:1 的比例随机分配因重症 COVID-19 肺炎住院的患者,接受单次静脉输注托珠单抗(剂量为 8mg/千克体重)或安慰剂。大约四分之一的参与者在首次给药后 8 至 24 小时接受了第二剂托珠单抗或安慰剂。主要结局是在改良意向治疗人群中,在第 28 天的临床状态,评分范围为 1(出院或准备出院)至 7(死亡),该人群包括至少接受一剂托珠单抗或安慰剂的所有患者。
在接受随机分组的 452 名患者中,438 名(托珠单抗组 294 名,安慰剂组 144 名)被纳入主要和次要分析。在第 28 天的排序量表上,托珠单抗组的临床状态中位数为 1.0(95%置信区间 [CI],1.0 至 1.0),安慰剂组为 2.0(非 ICU 住院,无需补充氧气)(95%CI,1.0 至 4.0)(组间差异,-1.0;95%CI,-2.5 至 0;van Elteren 检验 P=0.31)。在安全性人群中,托珠单抗组 295 名患者中有 103 名(34.9%)和安慰剂组 143 名患者中有 55 名(38.5%)发生严重不良事件。托珠单抗组第 28 天的死亡率为 19.7%,安慰剂组为 19.4%(加权差异,0.3 个百分点;95%CI,-7.6 至 8.2;名义 P=0.94)。
在这项涉及因重症 COVID-19 肺炎住院的患者的随机试验中,与安慰剂相比,使用托珠单抗在第 28 天时并未显著改善临床状态或降低死亡率。(由 F. Hoffmann-La Roche 和美国卫生与公众服务部资助;COVACTA ClinicalTrials.gov 编号,NCT04320615。)