Huang Ling-Ling, Yu Xue-Ping, Li Ju-Lan, Lin Hui-Ming, Kang Na-Ling, Jiang Jia-Ji, Zhu Yue-Yong, Liu Yu-Rui, Zeng Da-Wu
Department of Hepatology, Hepatology Research Institute, The First Affiliated Hospital, Fujian Medical University, Fuzhou 350005, Fujian Province, China.
Department of Infectious Diseases, The First Hospital of Quanzhou Affiliated to Fujian Medical University, Quanzhou 362000, Fujian Province, China.
World J Gastroenterol. 2021 Feb 21;27(7):641-653. doi: 10.3748/wjg.v27.i7.641.
Transient elastography (FibroScan) is a new and non-invasive test, which has been widely recommended by the guidelines of chronic hepatitis B virus (HBV) management for assessing hepatic fibrosis staging. However, some confounders may affect the diagnostic accuracy of the FibroScan device in fibrosis staging.
To evaluate the diagnostic value of the FibroScan device and the effect of hepatic inflammation on the accuracy of FibroScan in assessing the stage of liver fibrosis in patients with HBV infection.
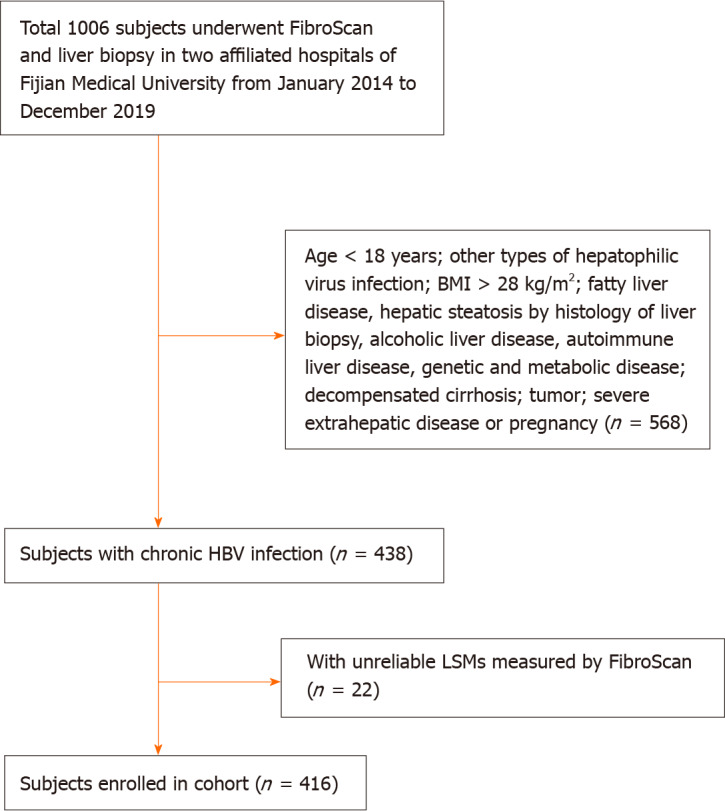
The data of 416 patients with chronic HBV infection who accepted FibroScan, liver biopsy, clinical, and biological examination were collected from two hospitals retrospectively. Receiver operating characteristic (ROC) curves were used to analyze the diagnostic performance of FibroScan for assessing the stage of liver fibrosis. Any discordance in fibrosis staging by FibroScan and pathological scores was statistically analyzed. Logistic regression and ROC analyses were used to analyze the accuracy of FibroScan in assessing the stage of fibrosis in patients with different degrees of liver inflammation. A non-invasive model was constructed to predict the risk of misdiagnosis of fibrosis stage using FibroScan.
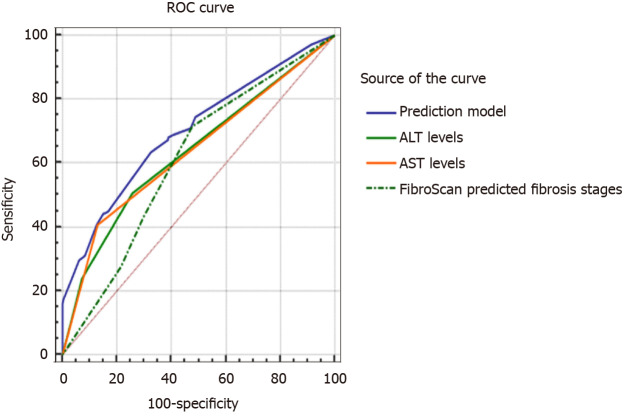
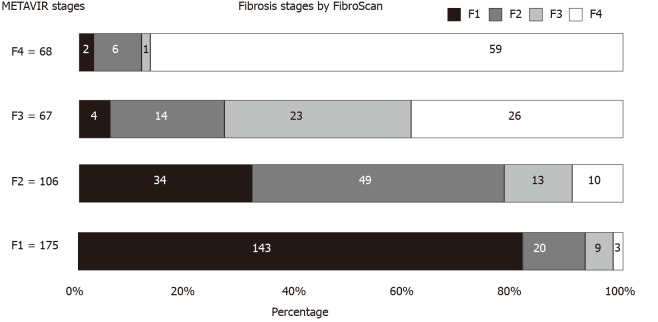
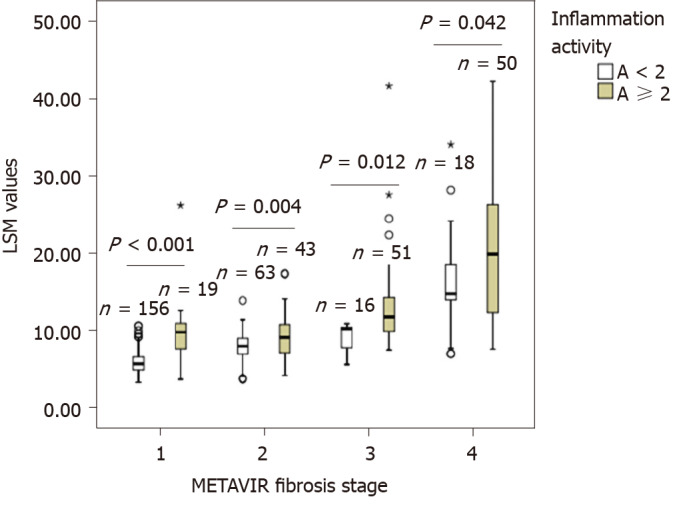
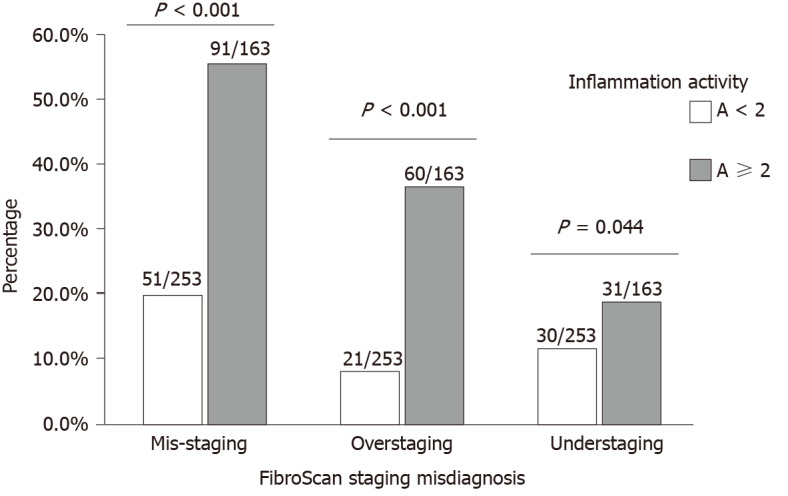
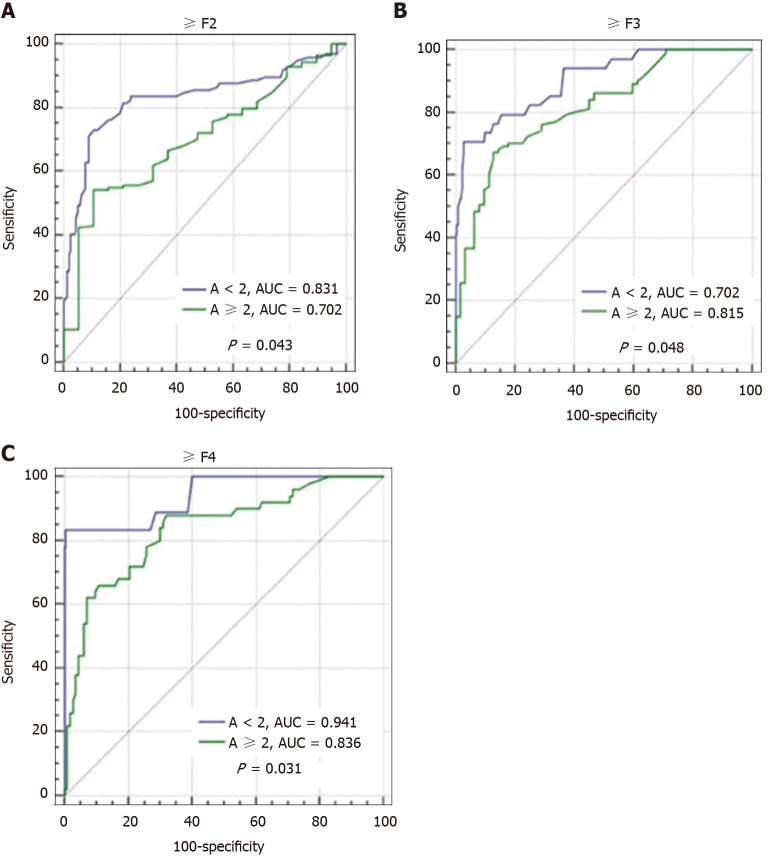
In the overall cohort, the optimal diagnostic values of liver stiffness measurement (LSM) using FibroScan for significant fibrosis (≥ F2), severe fibrosis (≥ F3), and cirrhosis (F4) were 7.3 kPa [area under the curve (AUC) = 0.863], 9.7 kPa (AUC = 0.911), and 11.3 kPa (AUC = 0.918), respectively. The rate of misdiagnosis of fibrosis stage using FibroScan was 34.1% (142/416 patients). The group of patients who showed discordance between fibrosis staging using FibroScan and pathological scores had significantly higher alanine aminotransferase and aspartate aminotransferase levels, and a higher proportion of moderate to severe hepatic inflammation, compared with the group of patients who showed concordance in fibrosis staging between the two methods. Liver inflammation activity over 2 (OR = 3.53) was an independent risk factor for misdiagnosis of fibrosis stage using FibroScan. Patients with liver inflammation activity ≥ 2 showed higher LSM values using FibroScan and higher rates of misdiagnosis of fibrosis stage, whereas the diagnostic performance of FibroScan for different fibrosis stages was significantly lower than that in patients with inflammation activity < 2 (all < 0.05). A non-invasive prediction model was established to assess the risk of misdiagnosis of fibrosis stage using FibroScan, and the AUC was 0.701.
Liver inflammation was an independent risk factor affecting the diagnostic accuracy of FibroScan for fibrosis stage. A combination of other related non-invasive factors can predict the risk of misdiagnosis of fibrosis staging using FibroScan.
瞬时弹性成像(FibroScan)是一项新型非侵入性检查,已被慢性乙型肝炎病毒(HBV)管理指南广泛推荐用于评估肝纤维化分期。然而,一些混杂因素可能会影响FibroScan设备在纤维化分期中的诊断准确性。
评估FibroScan设备的诊断价值以及肝脏炎症对FibroScan评估HBV感染患者肝纤维化分期准确性的影响。
回顾性收集两家医院416例接受FibroScan、肝活检、临床及生物学检查的慢性HBV感染患者的数据。采用受试者操作特征(ROC)曲线分析FibroScan评估肝纤维化分期的诊断性能。对FibroScan与病理评分在纤维化分期上的任何不一致进行统计学分析。采用逻辑回归和ROC分析来分析FibroScan在评估不同程度肝脏炎症患者纤维化分期中的准确性。构建一个非侵入性模型,以预测使用FibroScan误诊纤维化分期的风险。
在整个队列中,FibroScan测量肝脏硬度值(LSM)对显著纤维化(≥F2)、重度纤维化(≥F3)和肝硬化(F4)的最佳诊断值分别为7.3 kPa [曲线下面积(AUC)=0.863], 9.7 kPa(AUC =0.911)和11.3 kPa(AUC =0.918)。使用FibroScan误诊纤维化分期的比例为34.1%(142/416例患者)。与两种方法在纤维化分期上表现一致的患者组相比,FibroScan与病理评分在纤维化分期上表现不一致的患者组丙氨酸氨基转移酶和天冬氨酸氨基转移酶水平显著更高,中度至重度肝脏炎症的比例更高。肝脏炎症活动度超过2(OR =3.53)是使用FibroScan误诊纤维化分期的独立危险因素。肝脏炎症活动度≥2的患者使用FibroScan时LSM值更高,纤维化分期误诊率更高, 而FibroScan对不同纤维化分期的诊断性能显著低于炎症活动度<2的患者(均P<0.05)。建立了一个非侵入性预测模型来评估使用FibroScan误诊纤维化分期的风险,AUC为0.701。
肝脏炎症是影响FibroScan对纤维化分期诊断准确性的独立危险因素。其他相关非侵入性因素的组合可预测使用FibroScan误诊纤维化分期的风险。