Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, Minnesota.
Department of Health Sciences Research, Mayo Clinic, Rochester, Minnesota.
JAMA Netw Open. 2021 Mar 1;4(3):e210321. doi: 10.1001/jamanetworkopen.2021.0321.
There are limited data on the racial disparities in the incidence of attention-deficit/hyperactivity disorder (ADHD) diagnosis in children at the national level.
To explore differences in rates of diagnosis of ADHD and use of treatment among children by race and ethnicity.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study assessed insurance claims data of children born in the US between January 1, 2006, and December 31, 2012, who had continuous insurance coverage for at least 4 years. The last date of follow-up included in the cohort was June 30, 2019. Race/ethnicity designations were based on self-report and included non-Hispanic White, Black, Hispanic, and Asian. Data were analyzed between October 2019 and December 2020.
Race and ethnicity.
ADHD diagnosis as defined by International Classification of Diseases codes (ninth or tenth editions) and treatment within 1 year of diagnosis, including medication and behavior therapy as defined by billing codes. Data on ADHD diagnosis and treatment were adjusted for sex, region, and household income in a multivariate Cox regression model.
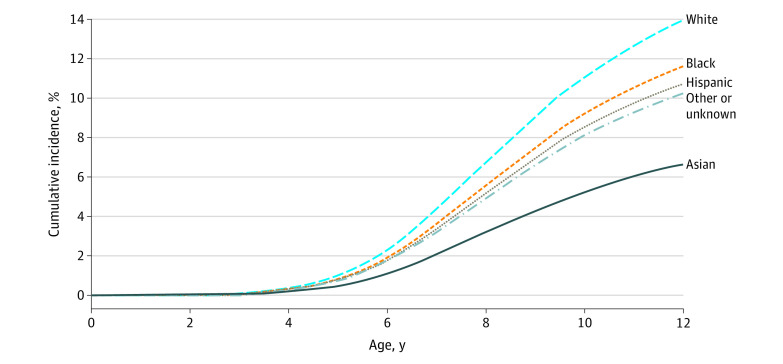
Among 238 011 children in the cohort (116 093 [48.8%] girls; 15 183 [6.7%] Asian, 14 792 [6.2%] Black, 23 358 [9.8%] Hispanic, and 173 082 [72.7%] White children), 11 401 (4.8%) were diagnosed with ADHD. The cumulative incidence at age 12 was 13.12% (95% CI, 12.79%-13.46%). In multivariate Cox regression adjusting for sex, region, and household income, the hazard ratio for Asian children was 0.48 (95% CI, 0.43-0.53); Black children, 0.83 (95% CI, 0.77-0.90); and Hispanic children, 0.77 (95% CI, 0.72, 0.82) compared with White children. In the first year after diagnosis, 516 preschool children (19.4%) received behavioral therapy only, 860 (32.4%) had medications only, 505 (19.0%) had both, and 774 (29.2%) had no claims associated with either option. A higher percentage of school-aged children (2904 [65.6%]) were prescribed medications, and fewer had therapy only (639 [14.4%]) or no treatment at all (884 [20.0%]). Compared with other groups, White children were more likely to receive some kind of treatment. Asian children had the highest odds of receiving no treatment (odds ratio compared with White children, 0.54; 95% CI, 0.42-0.70).
Racial and ethnic disparities in the diagnosis and treatment of ADHD are evident. Future study is needed to elucidate the mechanism behind these disparities, with special attention to Asian children. Clinicians should provide racially sensitive care in the evaluation and treatment of ADHD.
关于儿童注意缺陷多动障碍 (ADHD) 诊断在全国范围内的种族差异的数据有限。
探讨儿童 ADHD 诊断率和治疗使用率的种族和民族差异。
设计、地点和参与者:本回顾性队列研究评估了 2006 年 1 月 1 日至 2012 年 12 月 31 日期间在美国出生的儿童的保险索赔数据,这些儿童至少有 4 年的连续保险覆盖。队列中包含的最后随访日期为 2019 年 6 月 30 日。种族/民族分类基于自我报告,包括非西班牙裔白人、黑人、西班牙裔和亚洲人。数据分析于 2019 年 10 月至 2020 年 12 月进行。
种族和民族。
ADHD 诊断采用国际疾病分类 (第 9 或第 10 版) 定义,诊断后 1 年内的治疗包括按计费代码定义的药物治疗和行为治疗。在多变量 Cox 回归模型中,使用性别、地区和家庭收入对 ADHD 诊断和治疗数据进行了调整。
在队列中的 238011 名儿童中(116093 [48.8%] 为女孩;15183 [6.7%] 为亚洲人,14792 [6.2%] 为黑人,23358 [9.8%] 为西班牙裔,173082 [72.7%] 为白人儿童),有 11401 人(4.8%)被诊断为 ADHD。12 岁时的累积发病率为 13.12%(95%CI,12.79%-13.46%)。在多变量 Cox 回归中,按性别、地区和家庭收入调整后,亚洲儿童的危险比为 0.48(95%CI,0.43-0.53);黑人儿童为 0.83(95%CI,0.77-0.90);西班牙裔儿童为 0.77(95%CI,0.72, 0.82),与白人儿童相比。在诊断后的第一年,有 516 名学龄前儿童(19.4%)仅接受行为治疗,860 名(32.4%)仅接受药物治疗,505 名(19.0%)同时接受两种治疗,774 名(29.2%)未进行任何治疗。更多的学龄儿童(2904 名[65.6%])被开了药物,而接受单一疗法的儿童(639 名[14.4%])或根本没有治疗的儿童(884 名[20.0%])则较少。与其他群体相比,白人儿童更有可能接受某种治疗。亚洲儿童最不可能接受任何治疗(与白人儿童相比,比值比为 0.54;95%CI,0.42-0.70)。
ADHD 的诊断和治疗存在明显的种族和民族差异。未来需要进一步研究阐明这些差异背后的机制,特别关注亚洲儿童。临床医生应在 ADHD 的评估和治疗中提供种族敏感的护理。