Institute of Ecology and Environmental Sciences of Paris, Sorbonne Université, CNRS, UPEC, IRD, INRAE, Paris, France.
Center for Interdisciplinary Research in Biology, CNRS, Collège de France, PSL Research University, Paris, France.
PLoS Comput Biol. 2021 Mar 1;17(3):e1008752. doi: 10.1371/journal.pcbi.1008752. eCollection 2021 Mar.
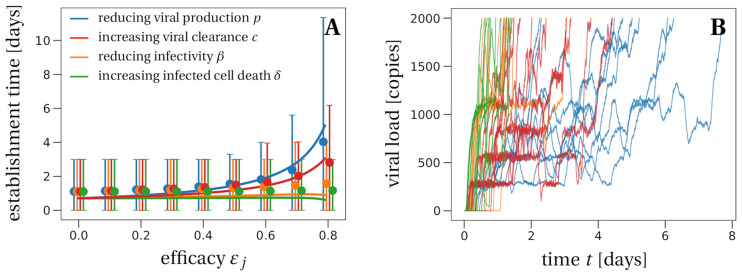
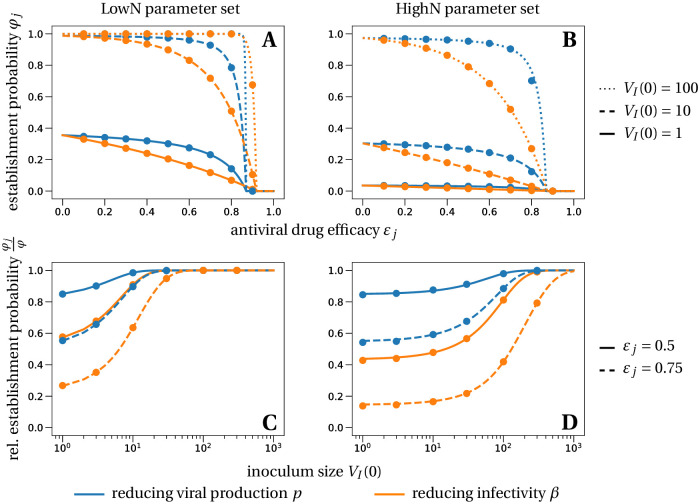
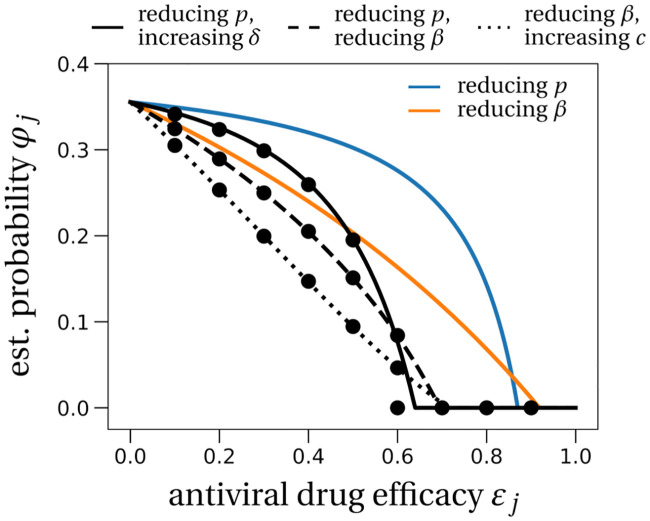
Repurposed drugs that are safe and immediately available constitute a first line of defense against new viral infections. Despite limited antiviral activity against SARS-CoV-2, several drugs are being tested as medication or as prophylaxis to prevent infection. Using a stochastic model of early phase infection, we evaluate the success of prophylactic treatment with different drug types to prevent viral infection. We find that there exists a critical efficacy that a treatment must reach in order to block viral establishment. Treatment by a combination of drugs reduces the critical efficacy, most effectively by the combination of a drug blocking viral entry into cells and a drug increasing viral clearance. Below the critical efficacy, the risk of infection can nonetheless be reduced. Drugs blocking viral entry into cells or enhancing viral clearance reduce the risk of infection more than drugs that reduce viral production in infected cells. The larger the initial inoculum of infectious virus, the less likely is prevention of an infection. In our model, we find that as long as the viral inoculum is smaller than 10 infectious virus particles, viral infection can be prevented almost certainly with drugs of 90% efficacy (or more). Even when a viral infection cannot be prevented, antivirals delay the time to detectable viral loads. The largest delay of viral infection is achieved by drugs reducing viral production in infected cells. A delay of virus infection flattens the within-host viral dynamic curve, possibly reducing transmission and symptom severity. Thus, antiviral prophylaxis, even with reduced efficacy, could be efficiently used to prevent or alleviate infection in people at high risk.
重新利用安全且可立即获得的药物是预防新病毒感染的第一道防线。尽管针对 SARS-CoV-2 的抗病毒活性有限,但仍有几种药物正在被测试作为药物或预防措施来预防感染。我们使用早期感染的随机模型,评估了不同药物类型预防病毒感染的预防性治疗的成功。我们发现,存在一个治疗必须达到的临界疗效,以阻止病毒建立。联合用药治疗可以降低临界疗效,最有效的是联合使用一种阻断病毒进入细胞的药物和一种增加病毒清除的药物。在临界疗效以下,仍可降低感染风险。阻断病毒进入细胞或增强病毒清除的药物比减少感染细胞中病毒产生的药物更能降低感染风险。初始感染病毒的接种量越大,预防感染的可能性就越小。在我们的模型中,我们发现只要病毒接种量小于 10 个感染性病毒颗粒,具有 90%(或更高)疗效的药物几乎可以肯定可以预防病毒感染。即使不能预防病毒感染,抗病毒药物也会延迟可检测到的病毒载量的时间。减少感染细胞中病毒产生的药物能最大程度地延迟病毒感染。病毒感染的延迟会使宿主内的病毒动态曲线变平,从而可能减少传播和症状严重程度。因此,即使疗效降低,抗病毒预防也可以有效地用于预防或减轻高危人群的感染。