The Centre for Health Services and Policy Research, School of Population and Public Health, The University of British Columbia, Vancouver, British Columbia, Canada.
British Columbia Centre for Disease Control, Vancouver, British Columbia, Canada.
PLoS One. 2021 Mar 1;16(3):e0247843. doi: 10.1371/journal.pone.0247843. eCollection 2021.
Sofosbuvir and ledipasvir-sofosbuvir are both newer direct-acting antiviral agents for the treatment of hepatitis C. The high list prices for both drugs have led to concern about the budget impact for public drug coverage programs. Therefore, we studied the impact of public prescription drug coverage for both drugs on utilization, adherence, and public and private expenditure in British Columbia, Canada.
We used provincial administrative claims data from January 2014 to June 2017 for all individuals historically tested for either hepatitis C and/or human immunodeficiency virus. Using interrupted time series analysis, we examined the impact of public insurance coverage on treatment uptake, adherence (proportion of days covered), and public and private expenditures.
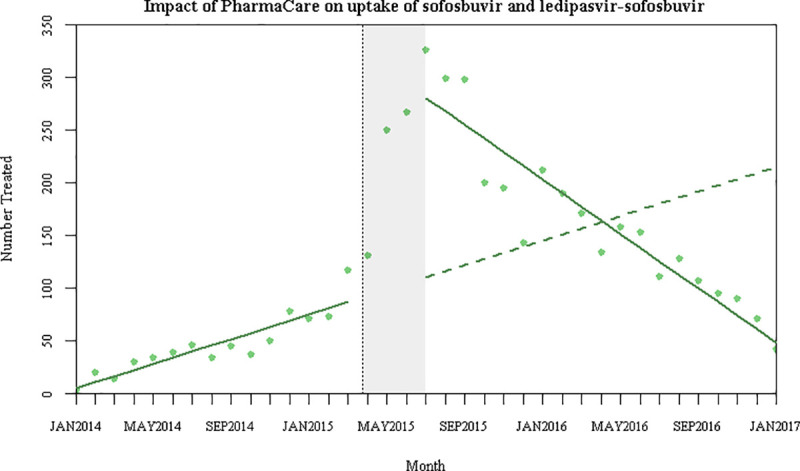
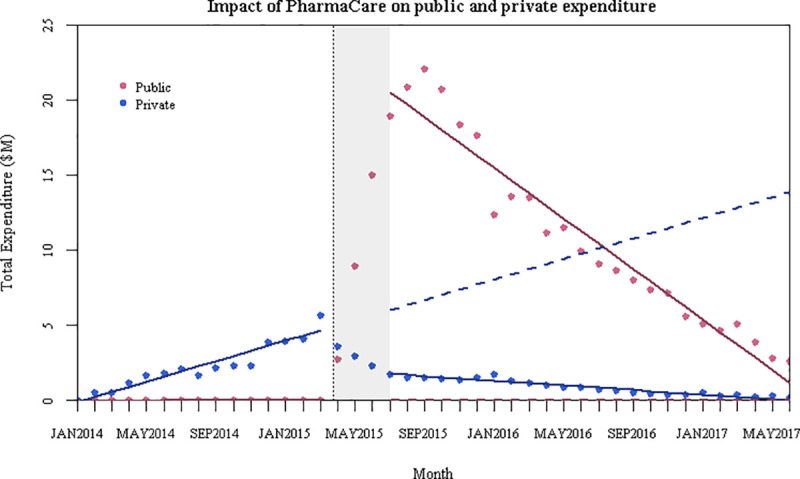
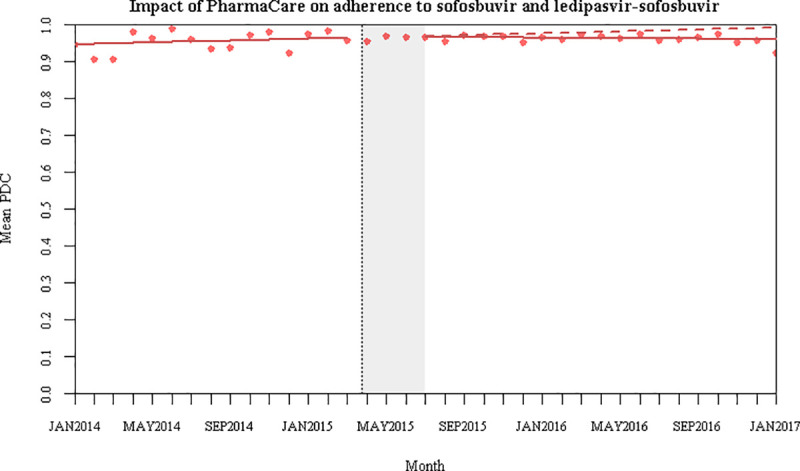
Over our study period, 4,462 treatment initiations were eligible for analysis (1,131 sofosbuvir and 3,331 ledipasvir-sofosbuvir, which include 19 patients initiated on both treatments). We found the start of public coverage for sofosbuvir and ledipasvir-sofosbuvir increased treatment uptake by 154%. Adherence rates were consistently high and did not change with public coverage. Finally, public expenditure increased after the policy change, and crowded out some private expenditure.
Public coverage for high-cost drugs for hepatitis C dramatically increased use of these drugs, but did not reduce adherence. From a health policy perspective, public payers should be prepared for increased treatment uptake following the availability of public coverage. However, they should not be concerned that populations without private insurance coverage will be less adherent and not finish their treatment course.
索非布韦和 ledipasvir-索非布韦都是新型直接作用抗病毒药物,用于治疗丙型肝炎。这两种药物的高昂标价引起了人们对公共药物覆盖项目预算影响的关注。因此,我们研究了不列颠哥伦比亚省(加拿大)公共处方药覆盖这两种药物对利用率、患者遵医嘱程度以及公共和私人支出的影响。
我们使用了 2014 年 1 月至 2017 年 6 月的省级行政索赔数据,涵盖了所有既往接受过丙型肝炎和/或人类免疫缺陷病毒检测的个体。我们采用中断时间序列分析,考察了公共保险覆盖对治疗开始、患者遵医嘱程度(覆盖天数比例)和公共及私人支出的影响。
在我们的研究期间,有 4462 例治疗开始符合分析条件(1131 例索非布韦和 3331 例 ledipasvir-索非布韦,其中包括 19 例同时开始这两种治疗的患者)。我们发现,索非布韦和 ledipasvir-索非布韦公共覆盖的开始使治疗开始增加了 154%。患者遵医嘱程度一直很高,并没有随着公共覆盖而改变。最后,政策变化后公共支出增加,挤出了一些私人支出。
丙型肝炎高成本药物的公共覆盖显著增加了这些药物的使用,但并没有降低患者的遵医嘱程度。从卫生政策角度来看,随着公共覆盖的提供,公共支付方应该为治疗人数的增加做好准备。然而,他们不必担心没有私人保险覆盖的人群会不遵医嘱且不能完成治疗疗程。