Genentech, Inc., South San Francisco, CA, United States of America.
Department of Population Health Sciences, Duke University School of Medicine, Durham, NC, United States of America.
PLoS One. 2023 Jan 19;18(1):e0280570. doi: 10.1371/journal.pone.0280570. eCollection 2023.
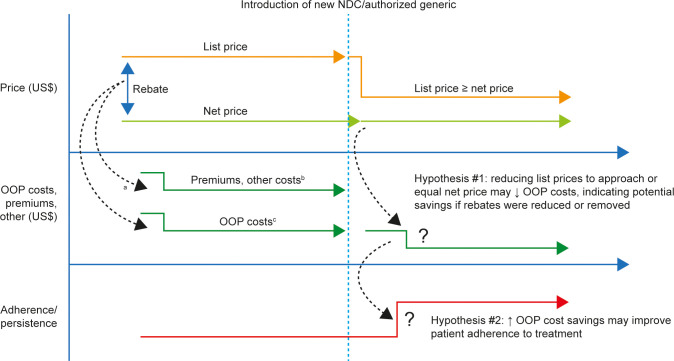
Insurers manage the cost of specialty medicines via rebates, however it is unclear if the savings are passed on to patients, and whether reducing rebates may lead to changes in patient out-of-pocket (OOP) costs and medication adherence. This study examined two drug classes to understand the impact of reducing list prices to net prices, via lower-priced national drug codes (NDCs) or authorized generics, on patient OOP costs and adherence.
This retrospective analysis assessed IQVIA PharMetrics ® Plus adjudicated medical and pharmacy claims for commercially insured patients. Patient OOP costs per prescription and payer drug costs were assessed for evolocumab or alirocumab (proprotein convertase subtilisin/kexin type 9 inhibitors [PCSK9is]) or velpatasvir/sofosbuvir or ledipasvir/sofosbuvir (hepatitis C virus [HCV] medications). For PCSK9is and HCV medications, the original and lower-priced versions were compared. Adherence was estimated based on proportion of days covered (PDC) (PCSK9is) and receipt of full treatment regimen (HCV medications).
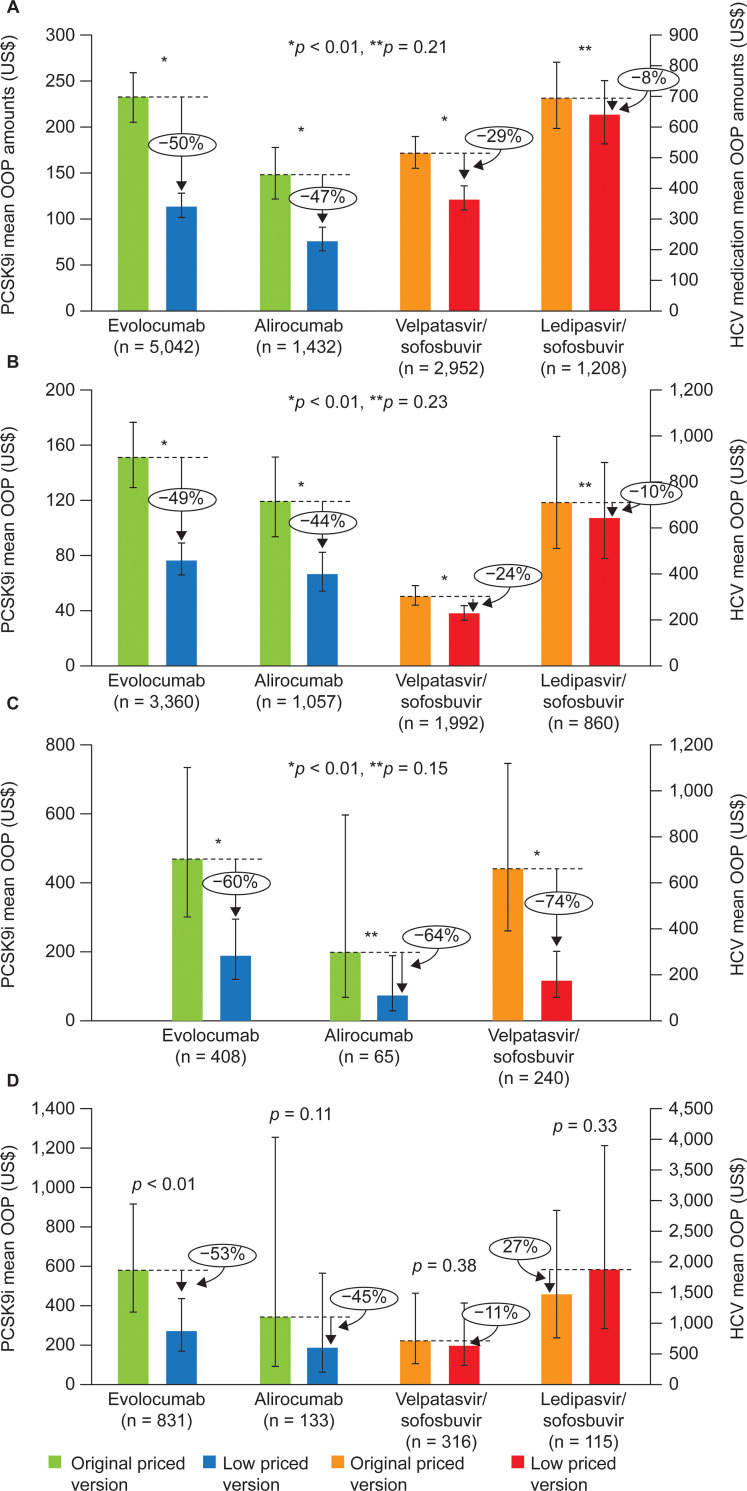
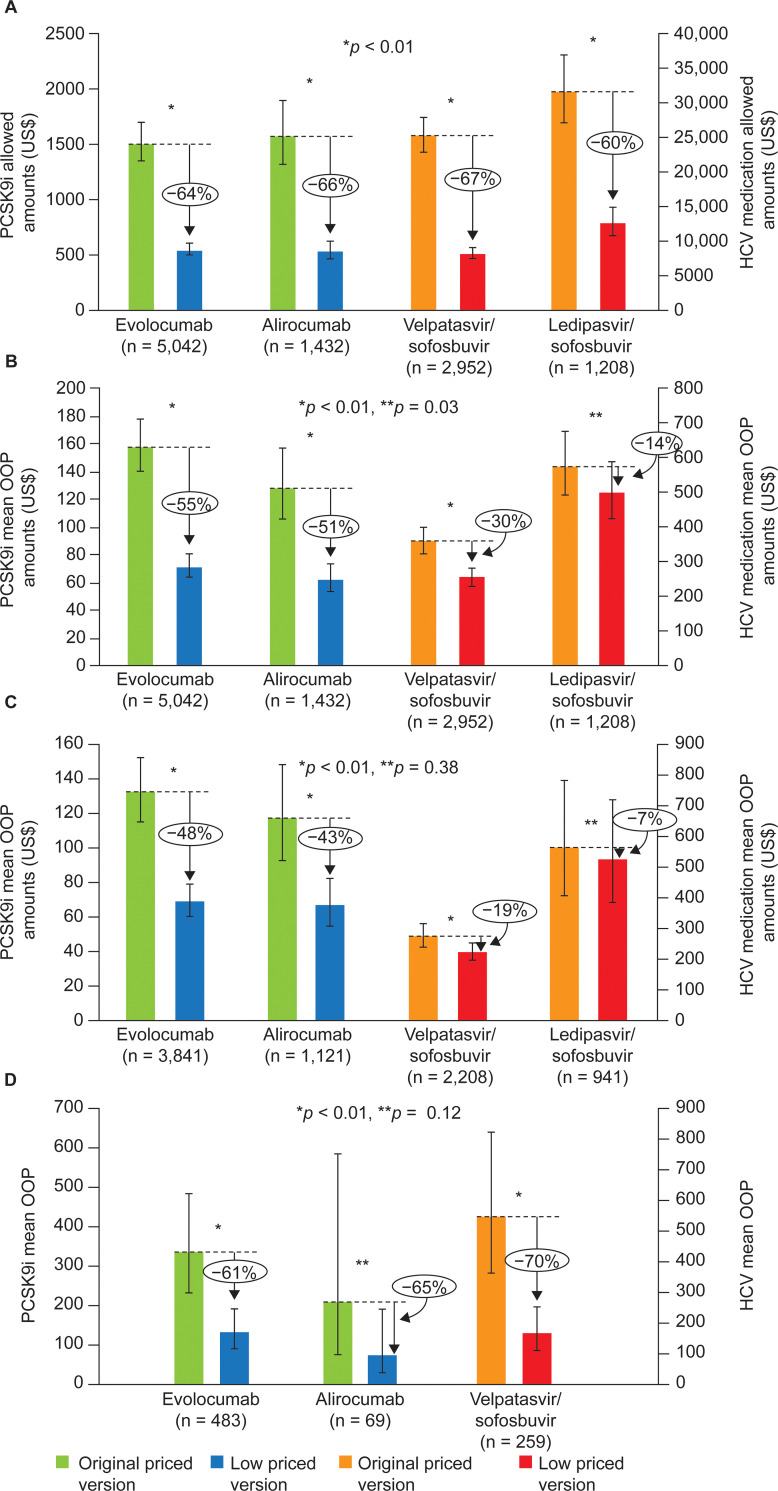
In total, 10,640 patients were included (evolocumab, 5,042; alirocumab, 1,438; velpatasvir/sofosbuvir, 2,952; ledipasvir/sofosbuvir,1,208). After list price reductions, mean payer drug costs decreased by over 60%, while patient OOP cost reductions ranged from 14% to 55% (evolocumab: 55%, p < 0.01; alirocumab: 51%, p < 0.01; velpatasvir/sofosbuvir: 30%, p < 0.01; ledipasvir/sofosbuvir: 14%, p = 0.03). Patients with coinsurance as the largest contributor to their OOP costs had the largest reductions in OOP costs, ranging from adjusted, mean values of US$135 to US$379 (>60% reductions). Six-month PDC for PCSK9is and proportion receiving full HCV treatment regimen were high with the original versions and did not substantially differ with the new, lower-priced versions.
Reducing list prices to approximate net prices (as a proxy for reducing rebates) resulted in lower patient OOP costs, particularly for those with coinsurance. Our findings suggest that future reduction of rebates may assist in patient affordability, although additional transparency is needed.
保险公司通过回扣来管理特种药物的成本,但目前尚不清楚这些节省是否转嫁给了患者,以及降低回扣是否会导致患者自付费用(OOP)和药物依从性的变化。本研究通过使用价格较低的国家药品代码(NDC)或授权仿制药,考察了两种药物类别,以了解降低标价至净价(以此来降低回扣)对患者 OOP 成本和药物依从性的影响。
本回顾性分析使用 IQVIA PharMetrics®Plus 评估了商业保险患者的医疗保险和药房理赔记录。使用 evolocumab 或 alirocumab(前蛋白转化酶枯草溶菌素 9 抑制剂[PCSK9i])或 velpatasvir/sofosbuvir 或 ledipasvir/sofosbuvir(丙型肝炎病毒[HCV]药物),评估患者每处方的 OOP 成本和支付方药物成本。对于 PCSK9i 和 HCV 药物,比较了原始和价格较低的版本。根据比例覆盖天数(PDC)(PCSK9i)和接受完整治疗方案(HCV 药物)来估计药物依从性。
共有 10640 名患者入选(evolocumab 5042 名,alirocumab 1438 名,velpatasvir/sofosbuvir 2952 名,ledipasvir/sofosbuvir 1208 名)。标价降低后,支付方药物成本平均降幅超过 60%,而患者 OOP 成本降幅在 14%至 55%之间(evolocumab:55%,p<0.01;alirocumab:51%,p<0.01;velpatasvir/sofosbuvir:30%,p<0.01;ledipasvir/sofosbuvir:14%,p=0.03)。OOP 成本中自付比例最大的患者 OOP 成本降幅最大,调整后的平均降幅为 135 美元至 379 美元(降幅超过 60%)。PCSK9i 的 6 个月 PDC 和接受完整 HCV 治疗方案的比例与原始版本相比均较高,且与新的、价格较低的版本相比没有显著差异。
将标价降低至近似净价(作为降低回扣的代理)可降低患者 OOP 成本,尤其是对那些自付比例较大的患者。我们的研究结果表明,未来降低回扣可能有助于提高患者的可负担性,但需要进一步提高透明度。