Aix Marseille Univ, INSERM, INRAE, C2VN, Marseille, France.
Department of Endocrinology, Metabolic Diseases and Nutrition, Pôle ENDO, APHM, Hôpital Nord, Chemin Des Bourrely, 13915, Marseille cedex 20, France.
Cardiovasc Diabetol. 2021 Mar 1;20(1):57. doi: 10.1186/s12933-021-01237-2.
Empagliflozin is a sodium-glucose cotransporter 2 (SGLT2) inhibitor that has demonstrated cardiovascular and renal protection in patients with type 2 diabetes (T2D). We hypothesized that empaglifozin (EMPA) could modulate ectopic fat stores and myocardial energetics in high-fat-high-sucrose (HFHS) diet mice and in type 2 diabetics (T2D).
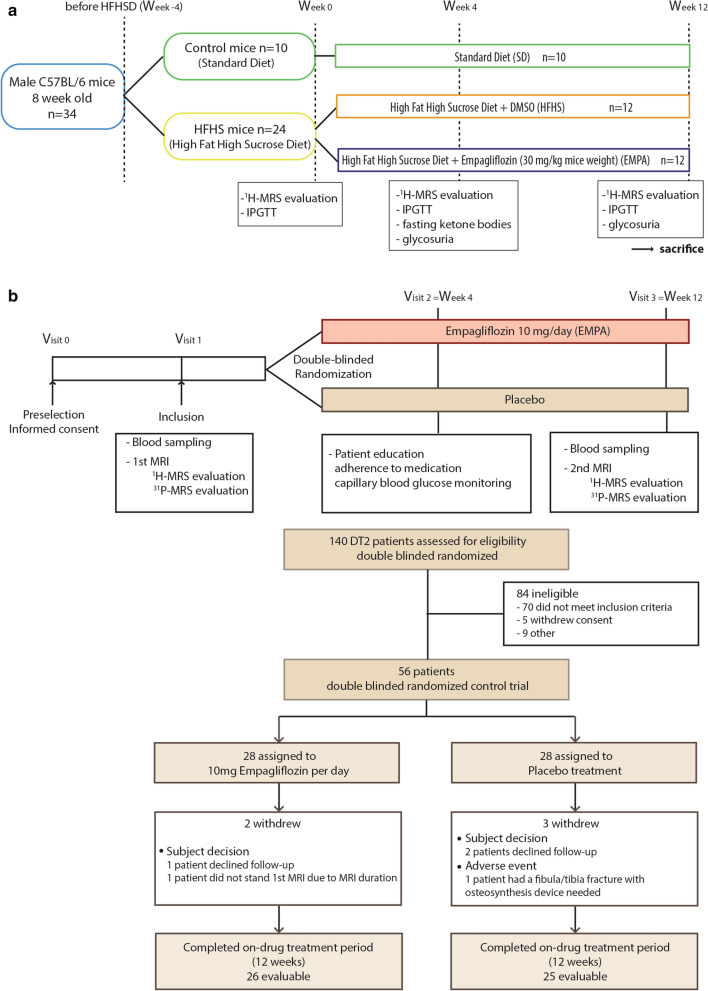
C57BL/6 HFHS mice (n = 24) and T2D subjects (n = 56) were randomly assigned to 12 weeks of treatment with EMPA (30 mg/kg in mice, 10 mg/day in humans) or with placebo. A 4.7 T or 3 T MRI with H-MRS evaluation-myocardial fat (primary endpoint) and liver fat content (LFC)-were performed at baseline and at 12 weeks. In humans, standard cardiac MRI was coupled with myocardial energetics (PCr/ATP) measured with P-MRS. Subcutaneous (SAT) abdominal, visceral (VAT), epicardial and pancreatic fat were also evaluated. The primary efficacy endpoint was the change in epicardial fat volume between EMPA and placebo from baseline to 12 weeks. Secondary endpoints were the differences in PCr/ATP ratio, myocardial, liver and pancreatic fat content, SAT and VAT between groups at 12 weeks.
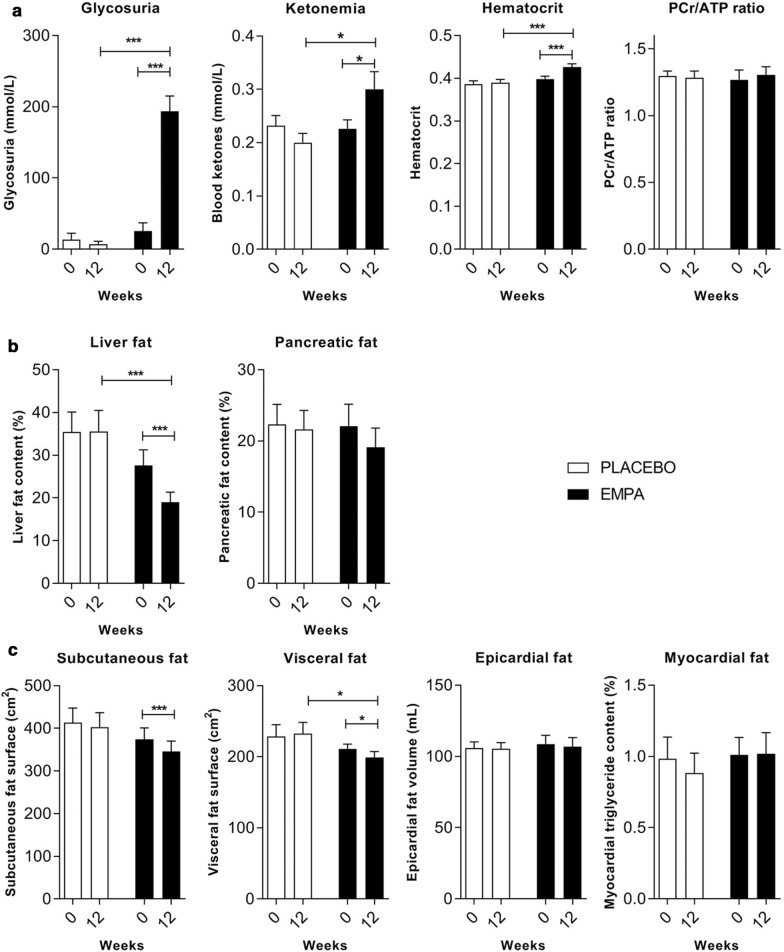
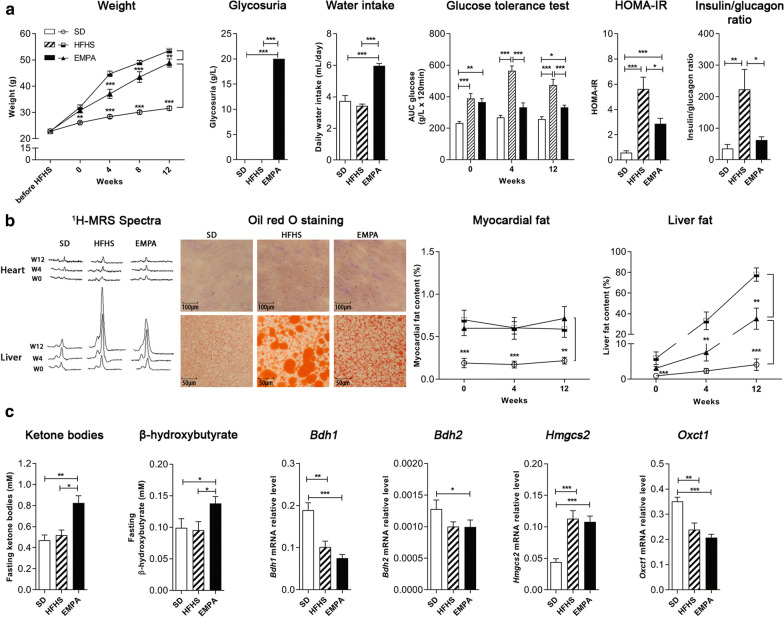
In mice fed HFHS, EMPA significantly improved glucose tolerance and increased blood ketone bodies (KB) and β-hydroxybutyrate levels (p < 0.05) compared to placebo. Mice fed HFHS had increased myocardial and liver fat content compared to standard diet mice. EMPA significantly attenuated liver fat content by 55%, (p < 0.001) but had no effect on myocardial fat. In the human study, all the 56 patients had normal LV function with mean LVEF = 63.4 ± 7.9%. Compared to placebo, T2D patients treated with EMPA significantly lost weight (- 2.6 kg [- 1.2; - 3.7]) and improved their HbA1c by 0.88 ± 0.74%. Hematocrit and EPO levels were significantly increased in the EMPA group compared to placebo (p < 0.0001, p = 0.041). EMPA significantly increased glycosuria and plasma KB levels compared to placebo (p < 0.0001, p = 0.012, respectively), and significantly reduced liver fat content (- 27 ± 23 vs. - 2 ± 24%, p = 0.0005) and visceral fat (- 7.8% [- 15.3; - 5.6] vs. - 0.1% [- 1.1;6.5], p = 0.043), but had no effect on myocardial or epicardial fat. At 12 weeks, no significant change was observed in the myocardial PCr/ATP (p = 0.57 between groups).
EMPA effectively reduced liver fat in mice and humans without changing epicardial, myocardial fat or myocardial energetics, rebutting the thrifty substrate hypothesis for cardiovascular protection of SGLT2 inhibitors. Trial registration NCT, NCT03118336. Registered 18 April 2017, https://clinicaltrials.gov/ct2/show/NCT03118336.
恩格列净是一种钠-葡萄糖共转运蛋白 2(SGLT2)抑制剂,已证明可在 2 型糖尿病(T2D)患者中提供心血管和肾脏保护。我们假设恩格列净(EMPA)可以调节高脂肪高蔗糖(HFHS)饮食小鼠和 2 型糖尿病患者的异位脂肪储存和心肌能量代谢。
将 C57BL/6 HFHS 小鼠(n = 24)和 T2D 患者(n = 56)随机分为 EMPA(小鼠 30mg/kg,人类 10mg/天)或安慰剂治疗 12 周。基线和 12 周时进行 4.7T 或 3T MRI 结合 H-MRS 评估心肌脂肪(主要终点)和肝脂肪含量(LFC)。在人类中,标准心脏 MRI 与心肌能量(PCr/ATP)的 P-MRS 测量相结合。还评估了皮下(SAT)腹部、内脏(VAT)、心外膜和胰腺脂肪。主要疗效终点是 EMPA 和安慰剂从基线到 12 周时心外膜脂肪体积的变化。次要终点是 EMPA 和安慰剂组 12 周时 PCr/ATP 比值、心肌、肝和胰腺脂肪含量、SAT 和 VAT 的差异。
与安慰剂相比,HFHS 饮食的小鼠中,EMPA 可显著改善葡萄糖耐量并增加血液酮体(KB)和β-羟丁酸水平(p < 0.05)。HFHS 饮食的小鼠与标准饮食的小鼠相比,心肌和肝脂肪含量增加。EMPA 可使肝脂肪含量显著减少 55%(p < 0.001),但对心肌脂肪没有影响。在人类研究中,所有 56 名患者的左心室功能均正常,平均 LVEF = 63.4 ± 7.9%。与安慰剂相比,接受 EMPA 治疗的 T2D 患者体重显著减轻(-2.6kg[-1.2; -3.7]),HbA1c 降低 0.88 ± 0.74%。与安慰剂相比,EMPA 组的红细胞压积和 EPO 水平显著升高(p < 0.0001,p = 0.041)。与安慰剂相比,EMPA 可显著增加尿糖和血浆 KB 水平(p < 0.0001,p = 0.012),并显著降低肝脂肪含量(-27 ± 23%[-15.3; -5.6]与-2 ± 24%[-1.1;6.5],p = 0.0005)和内脏脂肪(-7.8%[-15.3; -5.6]与-0.1%[-1.1;6.5],p = 0.043),但对心肌或心外膜脂肪没有影响。12 周时,心肌 PCr/ATP 无显著变化(组间 p = 0.57)。
EMPA 可有效减少小鼠和人类的肝脂肪,而不改变心外膜、心肌脂肪或心肌能量代谢,反驳了 SGLT2 抑制剂对心血管保护的节俭底物假说。试验注册 NCT,NCT03118336。于 2017 年 4 月 18 日注册,https://clinicaltrials.gov/ct2/show/NCT03118336。