National Institute of Public Health, University of Southern Denmark, Studiestræde 6, 1455, Copenhagen K, Denmark.
Department of Clinical Medicine, Aalborg University, Aalborg, Denmark.
Int J Health Geogr. 2021 Mar 1;20(1):11. doi: 10.1186/s12942-021-00264-2.
The prevalence and incidence rate of atrial fibrillation (AF) increase worldwide and AF is a risk factor for more adverse cardiovascular diseases including stroke. Approximately 44% of AF cases cannot be explained by common individual risk factors and risk might therefore also be related to the environment. By studying geographical variation and clustering in risk of incident AF adjusted for socioeconomic position at an individual level, potential neighbourhood risk factors could be revealed.
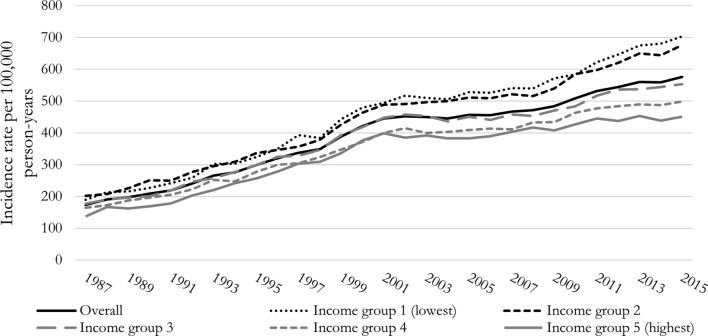
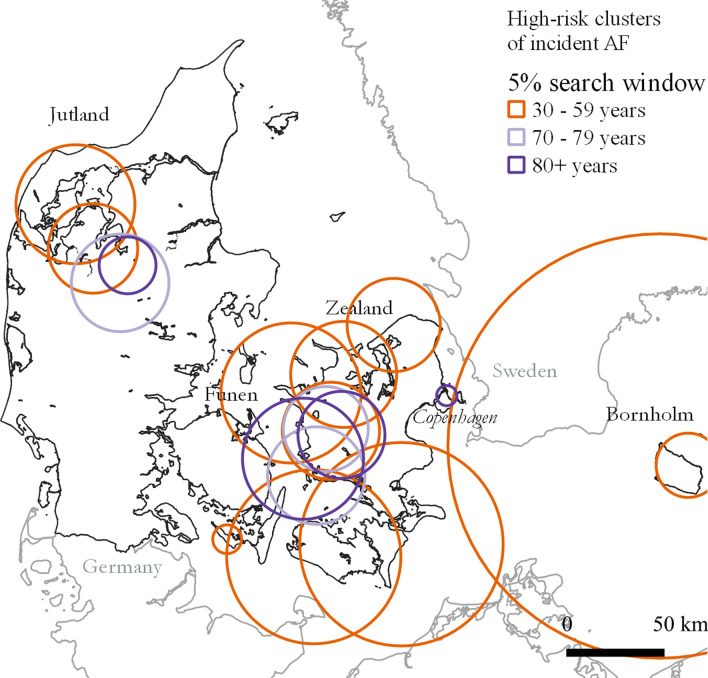
Initially, yearly AF incidence rates 1987-2015 were estimated overall and stratified by income in a register-based cohort study. To examine geographical variation and clustering in AF, we used both spatial scan statistics and a hierarchical Bayesian Poisson regression analysis of AF incidence rates with random effect of municipalities (n = 98) in Denmark in 2011-2015.
The 1987-2015 cohort included 5,453,639 individuals whereof 369,800 were diagnosed with an incident AF. AF incidence rate increased from 174 to 576 per 100,000 person-years from 1987 to 2015. Inequality in AF incidence rate ratio between highest and lowest income groups increased from 23% in 1987 to 38% in 2015. We found clustering and geographical variation in AF incidence rates, with incidence rates at municipality level being up to 34% higher than the country mean after adjusting for socioeconomic position.
Geographical variations and clustering in AF incidence rates exist. Compared to previous studies from Alberta, Canada and the United States, we show that geographical variations exist in a country with free access to healthcare and even when accounting for socioeconomic differences at an individual level. An increasing social inequality in AF was seen from 1987 to 2015. Therefore, when planning prevention strategies, attention to individuals with low income should be given. Further studies focusing on identification of neighbourhood risk factors for AF are needed.
心房颤动(AF)的患病率和发病率在全球范围内增加,AF 是包括中风在内的更多不良心血管疾病的危险因素。大约 44%的 AF 病例不能用常见的个体危险因素来解释,因此风险也可能与环境有关。通过研究个体水平上社会经济地位调整后的 AF 发病风险的地理差异和聚类,可以揭示潜在的邻里风险因素。
在一项基于登记的队列研究中,我们首先估计了 1987 年至 2015 年总体和按收入分层的 AF 年发病率。为了检查 AF 的地理差异和聚类,我们使用了空间扫描统计和 2011 年至 2015 年丹麦市(n=98)AF 发病率的分层贝叶斯泊松回归分析,具有市的随机效应。
1987 年至 2015 年的队列包括 5453639 人,其中 369800 人被诊断为新发 AF。1987 年至 2015 年,AF 发病率从 174 人/100000 人年增加到 576 人/100000 人年。最高和最低收入组之间 AF 发病率比值的不平等程度从 1987 年的 23%增加到 2015 年的 38%。我们发现 AF 发病率存在聚类和地理差异,调整社会经济地位后,市一级的发病率比全国平均水平高出 34%。
AF 发病率存在地理差异和聚类。与以前来自加拿大阿尔伯塔省和美国的研究相比,我们表明,在一个免费获得医疗保健的国家,甚至在考虑到个体层面的社会经济差异时,也存在地理差异。1987 年至 2015 年,AF 中社会不平等现象呈上升趋势。因此,在规划预防策略时,应关注低收入人群。需要进一步研究以确定 AF 的邻里风险因素。