Department of Clinical Science, Intervention and Technology, Division of Pediatrics, KI CLINTEC, Huddinge, Sweden
Allied Health Professionals Function, Occupational Therapy & Physiotherapy, Karolinska University Hospital, Stockholm, Sweden.
BMJ Open. 2021 Mar 2;11(3):e046407. doi: 10.1136/bmjopen-2020-046407.
The study aimed to investigate the heterogeneity of weight loss 5 years after Roux-en-Y gastric bypass (RYGB) and the association with cardiometabolic health as well as to model prediction estimates of surgical treatment failure.
Retrospective analysis of prospectively collected data from the Scandinavian Obesity Surgery Registry (SOReg).
29 surgical units from the whole of Sweden contributed data. Inclusion was restricted to surgical units with a retention rate of >60% five years postsurgery.
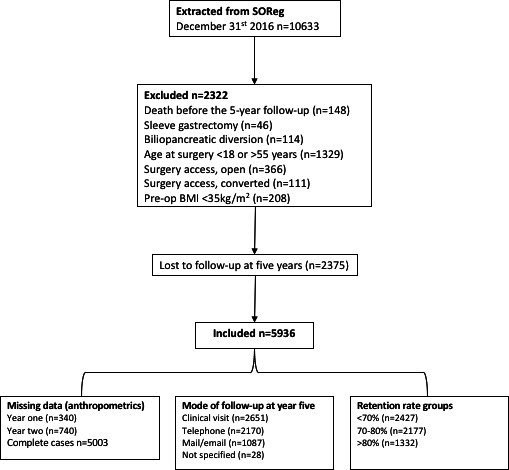
10 633 patients were extracted from SOReg. In total 5936 participants were included in the final sample, 79.1% females. The mean age of participants before surgery was 39.4±9 years and mean body mass index (BMI) 42.9±5.1. 2322 were excluded (death before the 5-year follow-up (n=148), other types of surgery or reoperations (n=637), age at surgery <18 or >55 years (n=1329), presurgery BMI <35 kg/m (n=208)). In total, 2375 (29%) of eligible individuals were lost to the 5-year follow-up.
The occurrence of surgical treatment failure 5 years after surgery was based on the three previously published definitions: per cent excess BMI loss <50%, total weight loss <20% or BMI >35 where initial BMI was <50, or >40 where initial BMI was >50. In addition, we report the association between surgical treatment failure and biochemical markers of obesity-related comorbidity. We also developed predictive models to identify patients with a high risk of surgical treatment failure 5 years postsurgery.
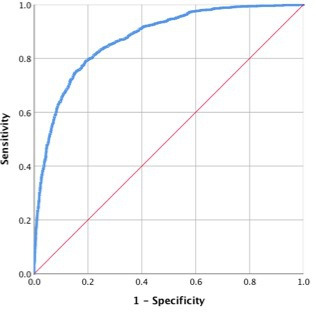
In total, 23.1% met at least one definition of surgical treatment failure at year 5 which was associated with (adjusted OR) with 95% CI): type 2 diabetes (T2D, OR 2.1; 95% CI 1.6 to 2.7), dyslipidaemia (OR 1.8; 95% CI 1.6 to 2.1) and hypertension (OR 1.9; 95% CI 1.6 to 2.2). Surgical treatment failure at 5 years was predicted by combined demographic and anthropometric measures from baseline, 1 and 2 years postsurgery (area under the curve=0.874).
Laparoscopic RYGB leads to a marked and sustained weight loss with improvement of obesity-related comorbidity in most patients. However, 23% met at least one definition of surgical treatment failure, which was associated with a greater risk of relapse and a higher incidence of T2D, dyslipidaemia and hypertension 5 years after surgery. Poor initial weight loss and early weight regain are strong predictors of long-term treatment failure and may be used for early identification of patients who require additional weight loss support.
本研究旨在探讨胃旁路手术后 5 年内体重减轻的异质性及其与心脏代谢健康的关系,并对手术治疗失败的预测估计进行建模。
对来自斯堪的纳维亚肥胖手术登记处(SOReg)的前瞻性收集数据进行回顾性分析。
来自瑞典各地的 29 个手术单位提供了数据。仅纳入手术后 5 年保留率>60%的手术单位。
从 SOReg 中提取了 10633 名患者。共有 5936 名参与者纳入最终样本,其中女性占 79.1%。参与者术前的平均年龄为 39.4±9 岁,平均 BMI 为 42.9±5.1。2322 人被排除在外(5 年随访前死亡(n=148),其他类型的手术或再次手术(n=637),手术时年龄<18 或>55 岁(n=1329),术前 BMI<35kg/m(n=208))。共有 2375 名(29%)符合条件的个体在 5 年随访中丢失。
根据之前发表的三种定义,术后 5 年手术治疗失败的发生率为:体重多余百分比减少<50%,总体重减轻<20%或 BMI>35,初始 BMI<50,或>40,初始 BMI>50。此外,我们报告了手术治疗失败与肥胖相关并发症的生化标志物之间的关联。我们还开发了预测模型来识别术后 5 年手术治疗失败风险较高的患者。
共有 23.1%的患者至少符合其中一项手术治疗失败的定义,与(调整后的 OR)95%置信区间相关:2 型糖尿病(T2D,OR 2.1;95%CI 1.6 至 2.7)、血脂异常(OR 1.8;95%CI 1.6 至 2.1)和高血压(OR 1.9;95%CI 1.6 至 2.2)。术后 5 年的手术治疗失败可通过基线、术后 1 年和 2 年的综合人口统计学和人体测量学指标预测(曲线下面积=0.874)。
腹腔镜胃旁路手术可显著且持续减轻体重,改善大多数患者的肥胖相关并发症。然而,23%的患者至少符合其中一项手术治疗失败的定义,这与术后 5 年复发风险增加以及 T2D、血脂异常和高血压的发生率较高相关。初始体重减轻不良和早期体重反弹是长期治疗失败的有力预测指标,可用于早期识别需要额外体重减轻支持的患者。