Department of Surgery, University of Michigan, Ann Arbor.
Center for Healthcare Outcomes and Policy, University of Michigan, Ann Arbor.
JAMA Netw Open. 2021 Mar 1;4(3):e210553. doi: 10.1001/jamanetworkopen.2021.0553.
Surgery is a teachable moment, and smoking cessation interventions that coincide with an episode of surgical care are especially effective. Implementing these interventions at a large scale requires understanding the prevalence and characteristics of smoking among surgical patients.
To describe the prevalence of smoking in a population of patients undergoing common surgical procedures and to identify any clinical or demographic characteristics associated with smoking.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study included all adult patients (aged ≥18 years) in a statewide registry who underwent general and vascular surgical procedures from 2012 to 2019 at 70 hospitals in Michigan. Data analysis was conducted from August to October 2020.
Undergoing a surgical procedure in any of the following categories: appendectomy, cholecystectomy, colon procedures, gastric or esophageal procedures, hepatopancreatobiliary procedures, hernia repair, small-bowel procedures, hysterectomy, vascular procedures, thyroidectomy, and other unspecific abdominal procedures.
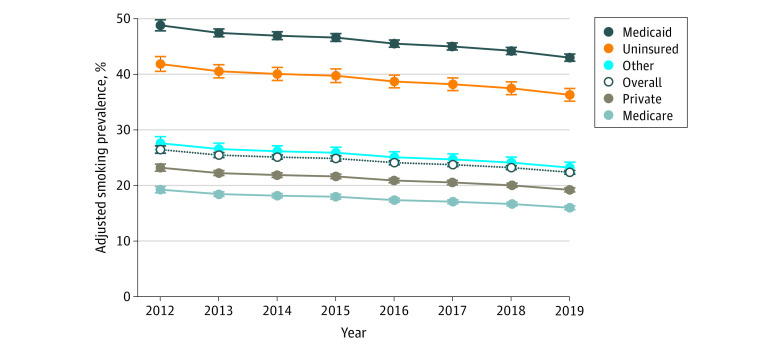
The prevalence of smoking prior to surgery, defined as cigarette use in the year prior to surgery, obtained from medical record review. Multivariable logistic regression was performed to analyze smoking prevalence based on insurance type and year of surgery while adjusting for demographic and clinical factors, including age, sex, race/ethnicity (determined from the medical record), insurance type, geographic region, comorbidities (ie, hypertension, diabetes, congestive heart failure, chronic obstructive pulmonary disease, chronic steroid use, and obstructive sleep apnea), American Society of Anesthesiologists classification, admission status, surgical priority, procedure type, and year of surgery.
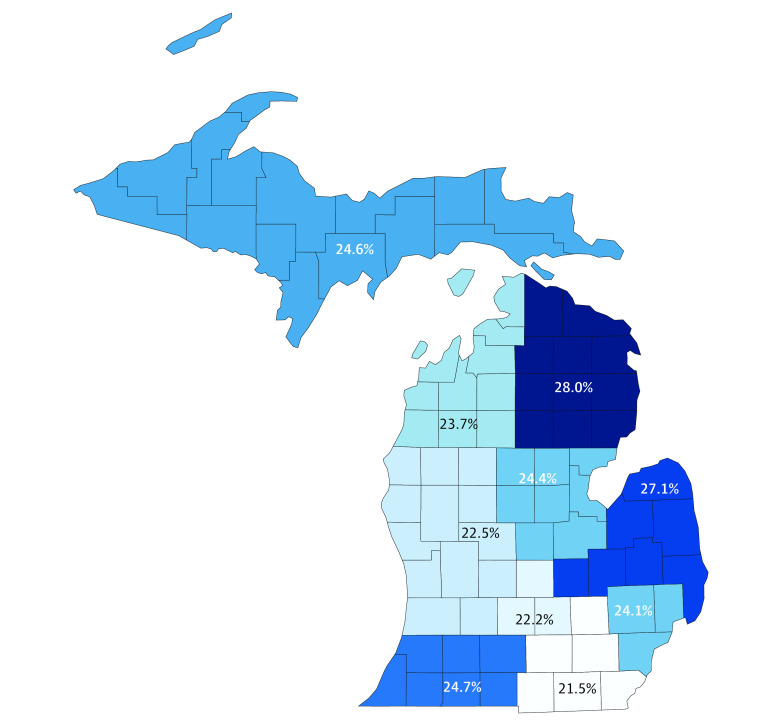
From 2012 to 2019, 328 578 patients underwent surgery and were included in analysis. Mean (SD) age was 54.0 (17.0) years, and 197 501 patients (60.1%) were women. The overall prevalence of smoking was 24.1% (79 152 patients). Prevalence varied regionally from 21.5% (95% CI, 21.0%-21.9%; 6686 of 31 172 patients) in southeast Michigan to 28.0% (95% CI, 27.1%-28.9%; 2696 of 9614 patients) in northeast Michigan. When adjusting for clinical and demographic factors, there were greater odds of smoking among patients with Medicaid (odds ratio [OR], 2.75; 95% CI, 2.69-2.82) and patients without insurance (OR, 2.21; 95% CI, 2.10-2.33) compared with patients with private insurance. Among procedure categories, patients undergoing vascular surgery had greater odds of smoking (OR, 3.24; 95% CI, 3.11-3.38) than those undergoing cholecystectomy. Compared with 2012, the adjusted odds of smoking decreased significantly each year (eg, 2019: OR, 0.78; 95% CI, 0.74-0.81). In 2019, the adjusted prevalence of smoking was 22.3% (95% CI, 22.0%-22.7%) among all patients, 43.0% (95% CI, 42.4%-43.6%) among patients with Medicaid, and 36.3% (95% CI, 35.2%-37.4%) among patients without insurance.
In a statewide population of surgical patients, nearly one-quarter of patients smoked cigarettes, which is higher than the national average. The prevalence of smoking was especially high among patients without insurance and among those receiving Medicaid. Given the established association between undergoing a major surgical procedure and health behavior change, targeted smoking cessation interventions at the time of surgery may be an effective strategy to improve population health, especially among at-risk patient groups.
手术是一个可以进行教育的时刻,与外科护理同时进行的戒烟干预措施尤其有效。要大规模实施这些干预措施,需要了解手术患者中吸烟的流行情况和特征。
描述在进行常见外科手术的患者人群中吸烟的流行情况,并确定与吸烟相关的任何临床或人口统计学特征。
设计、地点和参与者:这项横断面研究包括密歇根州 70 家医院在 2012 年至 2019 年期间接受普外科和血管外科手术的所有成年患者(年龄≥18 岁)。数据分析于 2020 年 8 月至 10 月进行。
接受以下任何一种手术类别:阑尾切除术、胆囊切除术、结肠手术、胃或食管手术、肝胆胰手术、疝修补术、小肠手术、子宫切除术、血管手术、甲状腺切除术和其他非特定腹部手术。
通过从病历中获取的手术前一年吸烟的定义(吸烟量)来衡量吸烟的流行情况。进行多变量逻辑回归分析,以根据保险类型和手术年份分析吸烟的流行情况,同时调整人口统计学和临床因素,包括年龄、性别、种族/民族(从病历中确定)、保险类型、地理区域、合并症(即高血压、糖尿病、充血性心力衰竭、慢性阻塞性肺疾病、慢性类固醇使用和阻塞性睡眠呼吸暂停)、美国麻醉医师协会分类、入院状态、手术优先级、手术类型和手术年份。
2012 年至 2019 年期间,有 328578 名患者接受了手术并纳入了分析。平均(标准差)年龄为 54.0(17.0)岁,197501 名患者(60.1%)为女性。吸烟的总体流行率为 24.1%(79152 名患者)。地域差异很大,从密歇根州东南部的 21.5%(95%CI,21.0%-21.9%;31172 名患者中的 6686 名)到密歇根州东北部的 28.0%(95%CI,27.1%-28.9%;9614 名患者中的 2696 名)。在调整临床和人口统计学因素后,与拥有私人保险的患者相比,拥有医疗补助的患者(比值比[OR],2.75;95%CI,2.69-2.82)和没有保险的患者(OR,2.21;95%CI,2.10-2.33)更有可能吸烟。在手术类别中,与胆囊切除术相比,接受血管手术的患者吸烟的可能性更高(OR,3.24;95%CI,3.11-3.38)。与 2012 年相比,每年吸烟的调整后几率显著下降(例如,2019 年:OR,0.78;95%CI,0.74-0.81)。2019 年,所有患者的吸烟调整后流行率为 22.3%(95%CI,22.0%-22.7%),医疗补助患者为 43.0%(95%CI,42.4%-43.6%),没有保险的患者为 36.3%(95%CI,35.2%-37.4%)。
在全州的外科患者人群中,近四分之一的患者吸烟,这高于全国平均水平。没有保险的患者和接受医疗补助的患者的吸烟率尤其高。鉴于进行重大手术与健康行为改变之间的既定关联,在手术时进行有针对性的戒烟干预可能是改善人群健康的有效策略,尤其是在高危患者群体中。